Forehead reconstruction is a critical component of تأنيث الوجه الجراحة (FFS) and craniofacial procedures, aiming to achieve a harmonious and aesthetically pleasing facial contour. Among the most debated techniques are النوع الأول و Type 3 cranioplasty, each offering distinct approaches to reshaping the forehead. While النوع الأول يتضمن bone burring or shaving, النوع 3 requires a more complex قطع العظم والنكسة of the frontal sinus. Understanding the anatomical, functional, and aesthetic implications of these techniques is essential for both surgeons and patients to make informed decisions.
This guide explores the structural differences between Type 1 and Type 3 cranioplasty, their impact on bone thickness, frontal sinus anatomy, and how surgeons determine the most suitable approach for each patient. By the end, you will gain clarity on which technique aligns best with your anatomical needs and aesthetic goals.
جدول المحتويات
الأساس التشريحي: العظم الجبهي والجيوب الأنفية
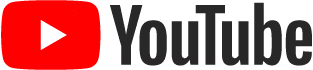
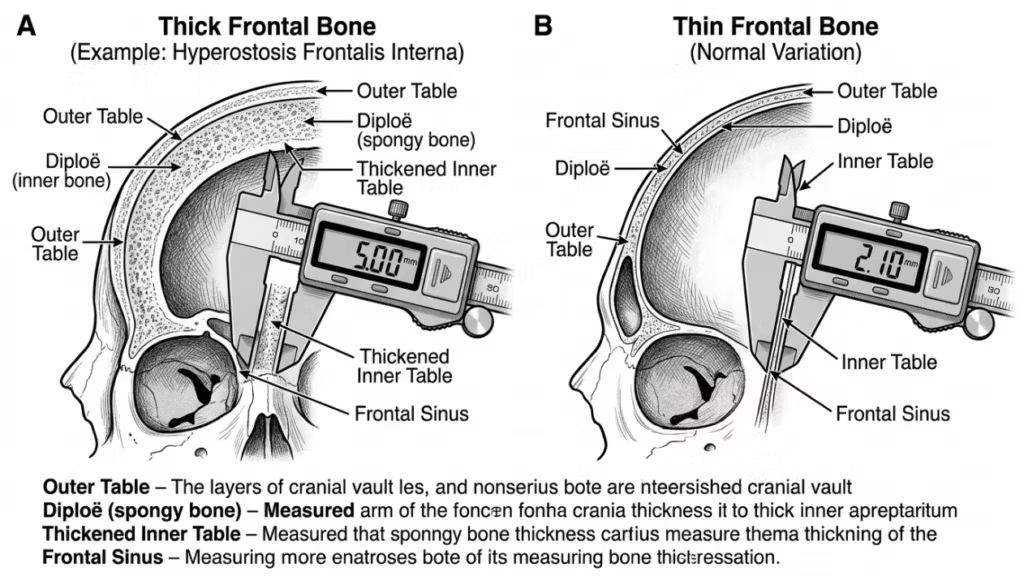
ال العظم الجبهي و frontal sinus play a pivotal role in forehead reconstruction. The frontal bone forms the upper part of the face and houses the frontal sinus, a hollow cavity that varies in size and shape among individuals. The anterior table of the frontal sinus is the outer layer of bone that contributes to the forehead’s contour, while the posterior table separates the sinus from the brain. The thickness of these tables and the degree of sinus pneumatization (air-filled expansion) influence the choice between Type 1 and Type 3 cranioplasty.
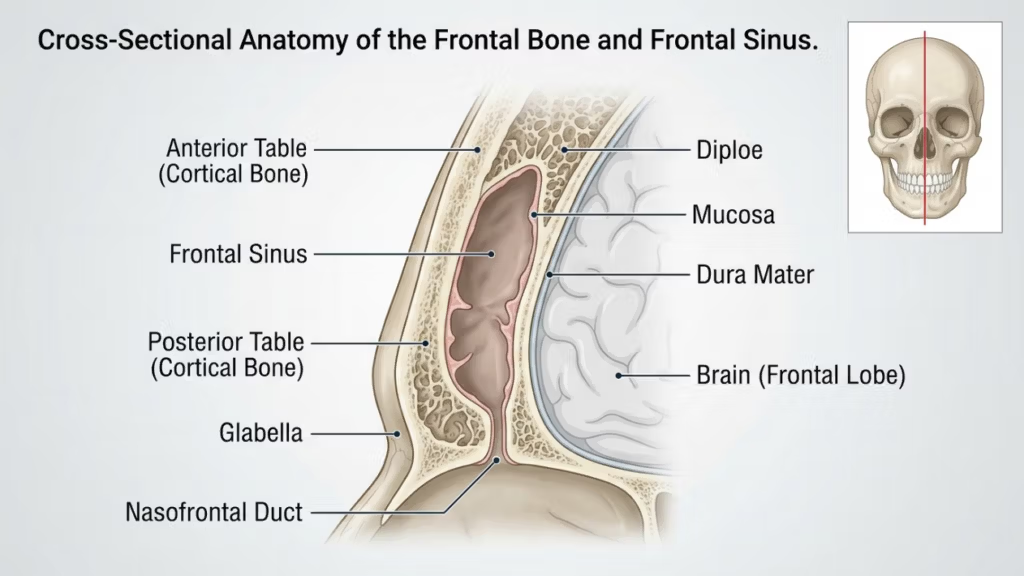
في Type 1 cranioplasty، ال دكتور جراح uses a high-speed burr to shave down the outer cortical bone, reducing prominence without violating the frontal sinus. This technique is ideal for patients with thin frontal bone or minimal bossing, as it preserves the sinus’s integrity. However, it may not be sufficient for patients with significant brow bossing or a thick anterior table, as excessive burring can compromise bone stability or fail to achieve the desired contour (Ousterhout, 2024).
In contrast, Type 3 cranioplasty involves an قطع العظم—a controlled cut through the anterior table of the frontal sinus. The bone segment is then repositioned backward (setback) to reduce projection and create a smoother, more feminine forehead. This technique is reserved for patients with moderate to severe brow bossing or a thick anterior table, where burring alone would be inadequate. The osteotomy allows for precise reshaping while maintaining the sinus’s protective function (Feminization of the Forehead: A Scoping Literature Review, 2024).
رأب الجمجمة من النوع الأول: الحلاقة والتجريف
نظرة عامة على التقنية
Type 1 cranioplasty is the least invasive option for forehead reconstruction. It involves using a high-speed burr to gradually reduce the prominence of the frontal bone. The surgeon meticulously shaves the outer cortical layer, avoiding penetration into the frontal sinus. This technique is particularly effective for patients with:
- Mild to moderate brow bossing
- Thin frontal bone (less than 5 mm)
- Absence of significant frontal sinus pneumatization
The procedure is performed through a شق تاجي, which allows access to the forehead while minimizing visible scarring. The surgeon uses tactile feedback and visual cues to ensure uniform reduction without over-thinning the bone, which could lead to instability or contour irregularities.
مزايا عملية ترقيع الجمجمة من النوع الأول
Type 1 cranioplasty offers several benefits:
- Minimal Invasiveness: No osteotomy or bone removal reduces surgical trauma and recovery time.
- انخفاض خطر حدوث مضاعفات: Preserving the frontal sinus minimizes the risk of sinusitis, cerebrospinal fluid leaks, or mucocele formation.
- وقت تشغيل أقصر: The procedure typically takes 1–2 hours, making it a quicker option compared to Type 3.
- Predictable Results: Ideal for patients with mild bossing, where subtle contouring is sufficient to achieve a feminine appearance.
محددات عملية ترقيع الجمجمة من النوع الأول
While Type 1 cranioplasty is safer and less invasive, it has notable limitations:
- Limited Reduction: Insufficient for patients with severe brow bossing or thick frontal bones.
- Risk of Over-Thinning: Aggressive burring can weaken the bone, leading to contour irregularities or fractures.
- التأنيث غير المكتمل: May not achieve the desired aesthetic outcome for patients with pronounced masculine features.
رأب الجمجمة من النوع الثالث: قطع العظم والتراجع
نظرة عامة على التقنية
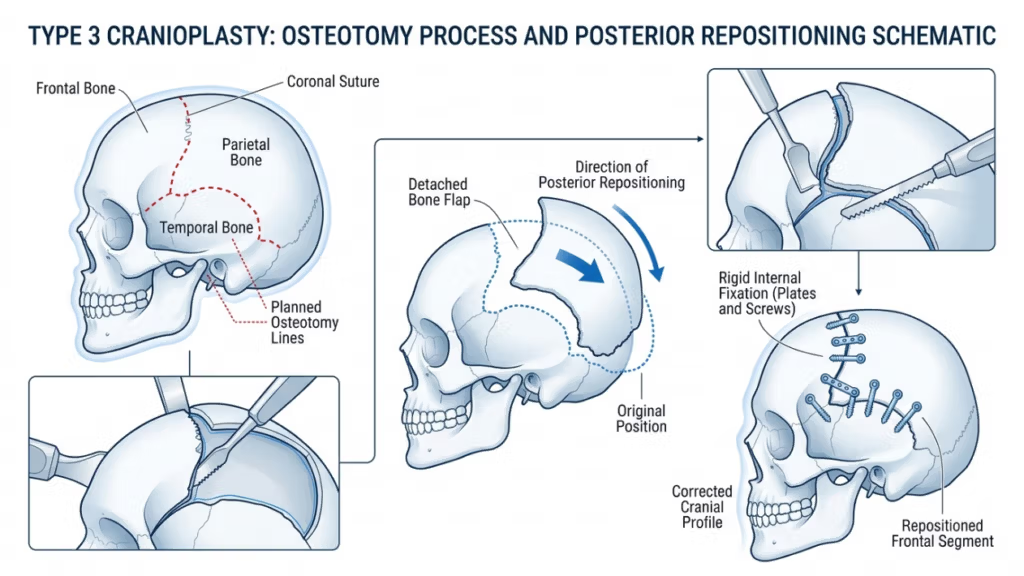
Type 3 cranioplasty is a more complex procedure designed for patients with moderate to severe brow bossing or thick frontal bones. It involves an قطع العظم—a precise cut through the anterior table of the frontal sinus—followed by repositioning the bone segment backward (setback). This technique allows for significant reduction in forehead projection and a smoother, more feminine contour.
The procedure is typically performed through a شق تاجي, providing access to the frontal bone and sinus. The surgeon uses a sagittal saw or piezoelectric device to create the osteotomy, ensuring the cut follows the natural curvature of the forehead. The bone segment is then repositioned and secured with صفائح ومسامير من التيتانيوم or resorbable sutures. This technique is ideal for patients with:
- Severe brow bossing
- Thick frontal bone (greater than 5 mm)
- Significant frontal sinus pneumatization
Type 3 cranioplasty requires meticulous planning, often involving التخطيط الجراحي الافتراضي ثلاثي الأبعاد (VSP) to simulate the osteotomy and setback. This ensures precision and minimizes the risk of complications such as sinus violation or cerebrospinal fluid leaks (Virtual Surgical Planning in Facial Feminization of the Upper Face, 2025).
مزايا عملية ترقيع الجمجمة من النوع الثالث
Type 3 cranioplasty offers several advantages for patients with pronounced masculine features:
- Significant Contouring: Achieves dramatic reduction in brow bossing, creating a smoother, more feminine forehead.
- براعه: Suitable for patients with thick frontal bones or extensive sinus pneumatization.
- الاستقرار على المدى الطويل: The repositioned bone segment integrates well, reducing the risk of contour irregularities over time.
- التخصيص: Virtual surgical planning allows for precise, patient-specific adjustments to achieve optimal results.
محددات عملية ترقيع الجمجمة من النوع الثالث
Despite its effectiveness, Type 3 cranioplasty carries higher risks and complexities:
- Increased Surgical Time: The procedure typically takes 3–5 hours, requiring greater precision and expertise.
- ارتفاع خطر حدوث المضاعفات: Potential risks include sinusitis, cerebrospinal fluid leaks, or mucocele formation if the sinus is violated.
- فترة تعافي أطول: Patients may experience prolonged swelling and discomfort compared to Type 1 cranioplasty.
- يكلف: The use of advanced imaging and surgical tools increases the overall cost of the procedure.

الاختلافات الرئيسية بين رأب الجمجمة من النوع الأول والنوع الثالث
| ميزة | Type 1 Cranioplasty | جراحة رأب الجمجمة من النوع الثالث |
|---|---|---|
| تقنية | Bone burring/shaving | Osteotomy and setback |
| الغزوية | الحد الأدنى | معتدلة إلى عالية |
| المرشحون المثاليون | Mild to moderate brow bossing, thin frontal bone | Severe brow bossing, thick frontal bone |
| وقت الجراحة | 1–2 hours | 3–5 hours |
| وقت الانتعاش | 1-2 أسابيع | 3-6 أسابيع |
| Risk of Complications | قليل | معتدلة إلى عالية |
| يكلف | أدنى | أعلى |
| النتيجة الجمالية | Subtle contouring | Dramatic feminization |
كيف يقرر الجراحون: النوع الأول مقابل النوع الثالث
The choice between Type 1 and Type 3 cranioplasty depends on several factors, including the patient’s anatomical features, aesthetic goals، و surgical risks. Surgeons rely on a combination of clinical examination, التصوير ثلاثي الأبعاد، و patient consultation to determine the most appropriate technique.
1. التقييم التشريحي
The first step is evaluating the patient’s frontal bone thickness و frontal sinus anatomy. أ CT scan أو إعادة بناء ثلاثية الأبعاد provides detailed insights into:
- سمك العظام: Patients with thin frontal bones (less than 5 mm) are better suited for Type 1 cranioplasty, while those with thicker bones may require Type 3.
- Sinus Pneumatization: Extensive sinus pneumatization may necessitate Type 3 cranioplasty to avoid violating the sinus during burring.
- Degree of Bossing: Severe brow bossing often requires the dramatic reduction achievable only with Type 3 techniques.
2. الأهداف الجمالية
Patients’ aesthetic expectations play a crucial role in technique selection. Those seeking subtle feminization may opt for Type 1 cranioplasty, while individuals with pronounced masculine features often require the transformative results of Type 3. Surgeons discuss realistic outcomes based on the patient’s anatomy and desired changes.
3. المخاطر الجراحية والتعافي
Type 3 cranioplasty carries higher risks, including sinus complications, cerebrospinal fluid leaks، و prolonged recovery. Surgeons assess the patient’s overall health, tolerance for surgery, and willingness to adhere to postoperative care. Patients with medical conditions that increase surgical risks may be advised to consider Type 1 or alternative procedures.
4. التخطيط الجراحي الافتراضي (VSP)
Advancements in 3D virtual surgical planning have revolutionized cranioplasty. Surgeons use VSP to simulate osteotomies, setbacks, and outcomes, ensuring precision and minimizing risks. This technology is particularly valuable for Type 3 cranioplasty, where accurate bone repositioning is critical (3D Printing and Virtual Surgical Planning in Craniofacial and Orthognathic Surgery, 2025).
الرعاية والتعافي بعد الجراحة
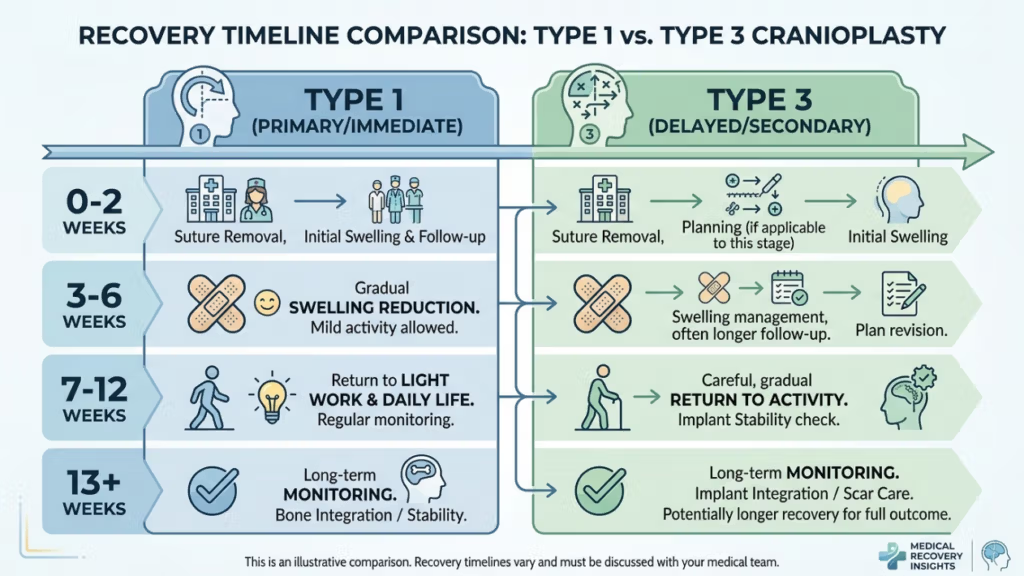
Recovery varies significantly between Type 1 and Type 3 cranioplasty. Understanding the postoperative process helps patients prepare for a smooth healing journey.
التعافي من عملية ترقيع الجمجمة من النوع الأول
Patients undergoing Type 1 cranioplasty typically experience:
- Mild to Moderate Swelling: Resolves within 1–2 weeks.
- Minimal Discomfort: Managed with over-the-counter pain medications.
- العودة السريعة إلى الأنشطة: Most patients resume normal activities within 2 weeks.
التعافي من عملية ترقيع الجمجمة من النوع الثالث
Recovery from Type 3 cranioplasty is more involved due to the complexity of the procedure:
- تورم كبير وكدمات: May persist for 3–4 weeks.
- Moderate Pain: Prescription pain medications may be required for the first week.
- العودة التدريجية للأنشطة: Strenuous activities are restricted for 4–6 weeks.
- زيارات المتابعة: Regular monitoring to ensure proper healing and address any complications.
Both techniques require patients to avoid heavy lifting, تمرين شاق، و direct pressure on the forehead during the initial recovery phase. Surgeons provide detailed postoperative instructions, including wound care, activity restrictions, and signs of complications to watch for.
المضاعفات المحتملة وكيفية تجنبها
While cranioplasty is generally safe, complications can arise. Awareness of these risks and preventive measures is crucial for both surgeons and patients.
المضاعفات الشائعة
- التهاب الجيوب الأنفية: Inflammation or infection of the frontal sinus, particularly in Type 3 cranioplasty if the sinus is violated.
- تسرب السائل النخاعي (CSF): Rare but serious complication if the posterior table of the sinus is breached.
- المخالفات الكنتورية: Over-thinning of bone in Type 1 or improper setback in Type 3 can lead to asymmetry or visible ridges.
- تكوين الخصية المخاطية: Blockage of sinus drainage pathways can result in mucus-filled cysts.
- عدوى: Risk is higher in Type 3 due to the longer operative time and use of implants.
التدابير الوقائية
Surgeons employ several strategies to minimize complications:
- التخطيط الجراحي الدقيق: 3D imaging and virtual surgical planning ensure accurate osteotomies and setbacks.
- Sinus Preservation: Avoiding violation of the frontal sinus during burring or osteotomy.
- Antibiotic Prophylaxis: Administered pre- and postoperatively to reduce infection risks.
- المراقبة بعد الجراحة: Regular follow-ups to detect early signs of complications.
- تثقيف المريض: Instructing patients on proper wound care, activity restrictions, and warning signs of complications.
بدائل لعملية ترقيع الجمجمة من النوع الأول والنوع الثالث
For patients who are not ideal candidates for Type 1 or Type 3 cranioplasty, alternative techniques may be considered:
- تطعيم الدهون: Autologous fat transfer can soften forehead contours without altering bone structure. This is ideal for patients with mild irregularities or those seeking non-surgical options.
- Custom Implants: Pre-fabricated implants, such as PEEK (polyether ether ketone) أو titanium, can be used to augment or reshape the forehead without osteotomy. These are particularly useful for patients with thin bones or sinus complications.
- جراحة تقويم الفكين: In cases where شد الجبين is part of a broader facial feminization plan, orthognathic procedures (e.g., Le Fort I osteotomy) may be combined to address midface and jaw alignment.
- Endoscopic Techniques: Minimally invasive endoscopic approaches can reduce brow bossing with smaller incisions and faster recovery times.
شهادات المرضى والنتائج الواقعية
Real-world outcomes provide valuable insights into the effectiveness and satisfaction rates of Type 1 and Type 3 cranioplasty. Patient testimonials highlight the transformative impact of these procedures:
Case Study 1: Type 1 Cranioplasty
A 28-year-old transgender woman sought subtle feminization of her forehead. With a thin frontal bone and minimal bossing, she opted for Type 1 cranioplasty. The procedure achieved a smoother contour with minimal downtime. She reported high satisfaction, noting that the results aligned with her expectations for a natural, feminine appearance.
Case Study 2: Type 3 Cranioplasty
A 35-year-old transgender woman presented with severe brow bossing and a thick frontal bone. Type 3 cranioplasty was performed, involving osteotomy and setback. The dramatic reduction in forehead projection significantly feminized her facial features. While recovery took longer, she expressed immense satisfaction with the results, stating that the procedure “changed her life.”
Case Study 3: Revision Surgery
A 40-year-old patient initially underwent Type 1 cranioplasty but was dissatisfied with the subtle results. She later opted for Type 3 cranioplasty to achieve more dramatic feminization. The revision surgery successfully addressed her concerns, demonstrating the importance of selecting the right technique based on anatomical needs and aesthetic goals.
دور التخطيط الجراحي الافتراضي في جراحة تجميل الجمجمة
Virtual surgical planning (VSP) has become a game-changer in cranioplasty, particularly for Type 3 procedures. VSP allows surgeons to:
- Simulate Osteotomies: Precisely plan bone cuts and repositioning to achieve optimal contouring.
- Predict Outcomes: Visualize postoperative results and adjust the surgical plan accordingly.
- تقليل المخاطر: Avoid critical structures such as the frontal sinus and supraorbital nerves.
- Enhance Communication: Share 3D models with patients to set realistic expectations and improve informed consent.
Studies have shown that VSP reduces operative time, improves accuracy, and enhances patient satisfaction (3D Printing and Virtual Surgical Planning in Craniofacial and Orthognathic Surgery, 2025). It is now considered the gold standard for complex cranioplasty procedures.

أسئلة مكررة
ما هو الفرق الرئيسي بين رأب الجمجمة من النوع الأول والنوع الثالث؟
تتضمن عملية تجميل الجمجمة من النوع الأول كشط أو برد الطبقة الخارجية لعظم الجبهة لتقليل بروزها، بينما تتطلب عملية تجميل الجمجمة من النوع الثالث قطع العظم (استئصال العظم) وإرجاع جزء من عظم الجبهة إلى الخلف لتحقيق شكل أكثر وضوحًا. يُعد النوع الأول أقل توغلاً ومناسبًا للبروز البسيط إلى المتوسط، بينما يُستخدم النوع الثالث للبروز الشديد أو عظام الجبهة السميكة.
كيف يختار الجراحون بين النوع الأول والنوع الثالث من عملية ترقيع الجمجمة؟
يُقيّم الجراحون سُمك عظم الجبهة، ودرجة بروز الحاجب، وتشريح الجيوب الأنفية الأمامية للمريض باستخدام التصوير المقطعي المحوسب والتصوير ثلاثي الأبعاد. يُختار النوع الأول للعظام الرقيقة والبروز الطفيف، بينما يُفضّل النوع الثالث للعظام السميكة، والبروز الشديد، أو التوسع الكبير في الجيوب الأنفية. كما تؤثر أهداف المريض ومدى تحمّله للمخاطر الجراحية على القرار.
ما هي المخاطر المرتبطة بجراحة ترقيع الجمجمة من النوع الثالث؟
تُعدّ جراحة ترميم الجمجمة من النوع الثالث أكثر خطورةً نظرًا لتعقيدها، وتشمل هذه المخاطر التهاب الجيوب الأنفية، وتسرب السائل النخاعي، وعدم انتظام شكل الجمجمة، وتكوّن الكيس المخاطي، والعدوى. ويتم تقليل هذه المخاطر إلى أدنى حدّ من خلال التخطيط الجراحي الدقيق، والحفاظ على الجيوب الأنفية، والمتابعة بعد العملية. كما يتم توعية المرضى بالعلامات التحذيرية والرعاية اللاحقة لضمان التعافي السلس.
ما هي مدة فترة التعافي لعملية ترقيع الجمجمة من النوع الأول مقارنة بالنوع الثالث؟
يستغرق التعافي من عملية ترقيع الجمجمة من النوع الأول عادةً من أسبوع إلى أسبوعين، مع تورم طفيف وشعور بعدم الراحة. أما عملية ترقيع الجمجمة من النوع الثالث فتتطلب فترة نقاهة أطول تتراوح بين ثلاثة وستة أسابيع نظرًا لتعقيد الجراحة واحتمالية حدوث مضاعفات. يُنصح المرضى بتجنب الأنشطة المجهدة واتباع تعليمات ما بعد الجراحة بدقة.
هل يمكن لعملية ترقيع الجمجمة من النوع الأول أن تحقق نفس نتائج النوع الثالث؟
لا، يقتصر النوع الأول من جراحة تجميل الجمجمة على تعديل بسيط في شكل الوجه، وهو مثالي لحالات بروز الجمجمة البسيط إلى المتوسط. أما النوع الثالث، فيحقق نتائج أكثر وضوحًا في تجميل الوجه من خلال إعادة تموضع عظم الجبهة، مما يجعله مناسبًا لحالات بروز الجمجمة الشديد أو عظام الجبهة السميكة. ويعتمد اختيار النوع المناسب على احتياجات المريض التشريحية وأهدافه الجمالية.
ما هو دور التخطيط الجراحي الافتراضي في عملية ترقيع الجمجمة؟
يُمكّن التخطيط الجراحي الافتراضي الجراحين من محاكاة عمليات قطع العظم، والتنبؤ بالنتائج، وتقليل المخاطر عن طريق تجنب المناطق الحساسة كالجيوب الأنفية الأمامية. كما يُحسّن هذا التخطيط الدقة، ويُقلل وقت العملية، ويرفع مستوى رضا المريض من خلال توفير رؤية واضحة للخطة الجراحية والنتائج المتوقعة.
هل توجد بدائل غير جراحية لعملية تجميل الجمجمة لتأنيث الجبهة؟
نعم، تشمل البدائل غير الجراحية حقن الدهون لتنعيم ملامح الوجه، وزراعة غرسات مخصصة (مثل غرسات PEEK أو التيتانيوم) لإعادة تشكيل الجبهة دون الحاجة إلى قطع العظم. تُعد هذه الخيارات مثالية للمرضى الذين يعانون من عدم انتظام طفيف في ملامح الوجه أو الذين يفضلون تجنب الجراحة. مع ذلك، قد لا تحقق هذه البدائل نفس مستوى التأنيث الذي تحققه التقنيات الجراحية.
ما الذي يجب أن أتوقعه خلال الاستشارة الخاصة بإعادة بناء الجبهة؟
خلال الاستشارة، سيقوم الجراح بتقييم سُمك عظم الجبهة، وتشريح الجيوب الأنفية، ودرجة بروز الجمجمة باستخدام الفحص السريري والتصوير ثلاثي الأبعاد. سيناقش معك أهدافك التجميلية، ويشرح لك الفرق بين جراحة تجميل الجمجمة من النوع الأول والنوع الثالث، ويوصي بالتقنية الأنسب بناءً على تشريحك وتوقعاتك.