Forehead reconstruction is a critical component of Femminilizzazione facciale Chirurgia (FFS) and craniofacial procedures, aiming to achieve a harmonious and aesthetically pleasing facial contour. Among the most debated techniques are Tipo 1 E Type 3 cranioplasty, each offering distinct approaches to reshaping the forehead. While Tipo 1 involves bone burring or shaving, Digitare 3 requires a more complex osteotomia e arretramento of the frontal sinus. Understanding the anatomical, functional, and aesthetic implications of these techniques is essential for both surgeons and patients to make informed decisions.
This guide explores the structural differences between Type 1 and Type 3 cranioplasty, their impact on bone thickness, frontal sinus anatomy, and how surgeons determine the most suitable approach for each patient. By the end, you will gain clarity on which technique aligns best with your anatomical needs and aesthetic goals.
Sommario
Le basi anatomiche: osso frontale e seno mascellare
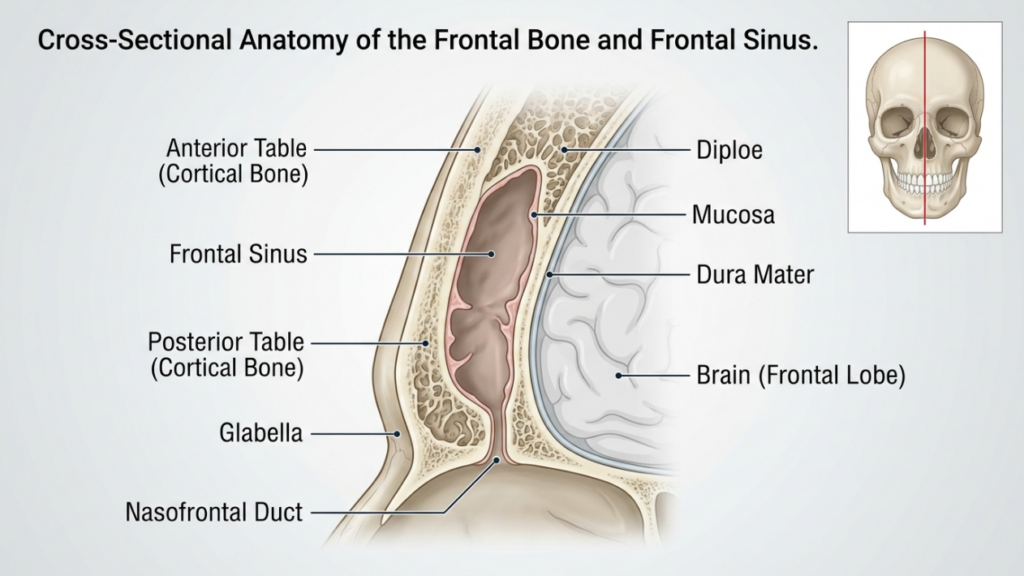
IL osso frontale E frontal sinus play a pivotal role in forehead reconstruction. The frontal bone forms the upper part of the face and houses the frontal sinus, a hollow cavity that varies in size and shape among individuals. The anterior table of the frontal sinus is the outer layer of bone that contributes to the forehead’s contour, while the posterior table separates the sinus from the brain. The thickness of these tables and the degree of sinus pneumatization (air-filled expansion) influence the choice between Type 1 and Type 3 cranioplasty.
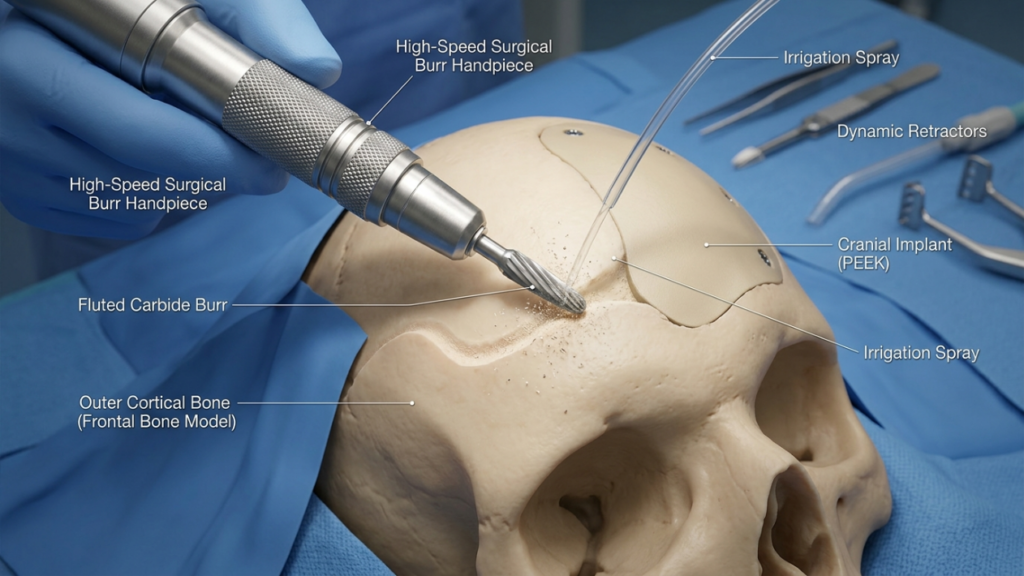
In Type 1 cranioplasty, IL chirurgo uses a high-speed burr to shave down the outer cortical bone, reducing prominence without violating the frontal sinus. This technique is ideal for patients with thin frontal bone or minimal bossing, as it preserves the sinus’s integrity. However, it may not be sufficient for patients with significant brow bossing or a thick anterior table, as excessive burring can compromise bone stability or fail to achieve the desired contour (Ousterhout, 2024).
In contrast, Type 3 cranioplasty involves an osteotomia—a controlled cut through the anterior table of the frontal sinus. The bone segment is then repositioned backward (setback) to reduce projection and create a smoother, more feminine forehead. This technique is reserved for patients with moderate to severe brow bossing or a thick anterior table, where burring alone would be inadequate. The osteotomy allows for precise reshaping while maintaining the sinus’s protective function (Feminization of the Forehead: A Scoping Literature Review, 2024).
Cranioplastica di tipo 1: rasatura e fresatura
Panoramica tecnica
Type 1 cranioplasty is the least invasive option for forehead reconstruction. It involves using a high-speed burr to gradually reduce the prominence of the frontal bone. The surgeon meticulously shaves the outer cortical layer, avoiding penetration into the frontal sinus. This technique is particularly effective for patients with:
- Mild to moderate brow bossing
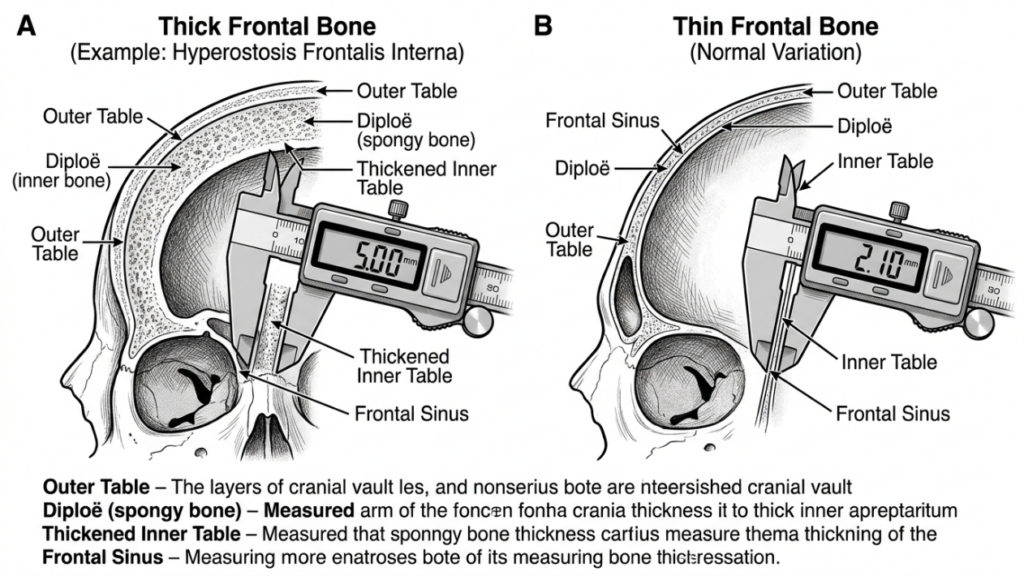
- Thin frontal bone (less than 5 mm)
- Absence of significant frontal sinus pneumatization
The procedure is performed through a incisione coronale, which allows access to the forehead while minimizing visible scarring. The surgeon uses tactile feedback and visual cues to ensure uniform reduction without over-thinning the bone, which could lead to instability or contour irregularities.
Vantaggi della cranioplastica di tipo 1
Type 1 cranioplasty offers several benefits:
- Minimal Invasiveness: No osteotomy or bone removal reduces surgical trauma and recovery time.
- Minor rischio di complicazioni: Preserving the frontal sinus minimizes the risk of sinusitis, cerebrospinal fluid leaks, or mucocele formation.
- Tempo operatorio più breve: The procedure typically takes 1–2 hours, making it a quicker option compared to Type 3.
- Predictable Results: Ideal for patients with mild bossing, where subtle contouring is sufficient to achieve a feminine appearance.
Limitazioni della cranioplastica di tipo 1
While Type 1 cranioplasty is safer and less invasive, it has notable limitations:
- Limited Reduction: Insufficient for patients with severe brow bossing or thick frontal bones.
- Risk of Over-Thinning: Aggressive burring can weaken the bone, leading to contour irregularities or fractures.
- Femminilizzazione incompleta: May not achieve the desired aesthetic outcome for patients with pronounced masculine features.
Cranioplastica di tipo 3: osteotomia e arretramento
Panoramica tecnica
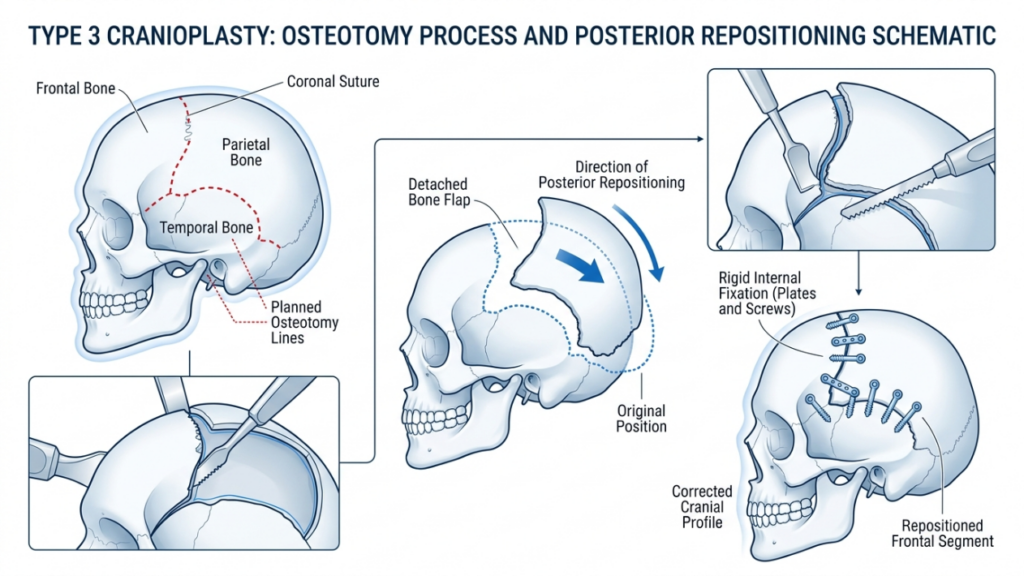
Type 3 cranioplasty is a more complex procedure designed for patients with moderate to severe brow bossing or thick frontal bones. It involves an osteotomia—a precise cut through the anterior table of the frontal sinus—followed by repositioning the bone segment backward (setback). This technique allows for significant reduction in forehead projection and a smoother, more feminine contour.
The procedure is typically performed through a incisione coronale, providing access to the frontal bone and sinus. The surgeon uses a sagittal saw or piezoelectric device to create the osteotomy, ensuring the cut follows the natural curvature of the forehead. The bone segment is then repositioned and secured with piastre e viti in titanio or resorbable sutures. This technique is ideal for patients with:
- Severe brow bossing
- Thick frontal bone (greater than 5 mm)
- Significant frontal sinus pneumatization
Type 3 cranioplasty requires meticulous planning, often involving Pianificazione chirurgica virtuale 3D (VSP) to simulate the osteotomy and setback. This ensures precision and minimizes the risk of complications such as sinus violation or cerebrospinal fluid leaks (Virtual Surgical Planning in Facial Feminization of the Upper Face, 2025).
Vantaggi della cranioplastica di tipo 3
Type 3 cranioplasty offers several advantages for patients with pronounced masculine features:
- Significant Contouring: Achieves dramatic reduction in brow bossing, creating a smoother, more feminine forehead.
- Versatilità: Suitable for patients with thick frontal bones or extensive sinus pneumatization.
- Stabilità a lungo termine: The repositioned bone segment integrates well, reducing the risk of contour irregularities over time.
- Personalizzazione: Virtual surgical planning allows for precise, patient-specific adjustments to achieve optimal results.
Limitazioni della cranioplastica di tipo 3
Despite its effectiveness, Type 3 cranioplasty carries higher risks and complexities:
- Increased Surgical Time: The procedure typically takes 3–5 hours, requiring greater precision and expertise.
- Rischio più elevato di complicazioni: Potential risks include sinusitis, cerebrospinal fluid leaks, or mucocele formation if the sinus is violated.
- Recupero più lungo: Patients may experience prolonged swelling and discomfort compared to Type 1 cranioplasty.
- Costo: The use of advanced imaging and surgical tools increases the overall cost of the procedure.

Principali differenze tra cranioplastica di tipo 1 e di tipo 3
| Caratteristica | Type 1 Cranioplasty | Cranioplastica di tipo 3 |
|---|---|---|
| Tecnica | Bone burring/shaving | Osteotomy and setback |
| Invasività | Minimo | Da moderato ad alto |
| Candidati ideali | Mild to moderate brow bossing, thin frontal bone | Severe brow bossing, thick frontal bone |
| Tempo chirurgico | 1–2 hours | 3–5 hours |
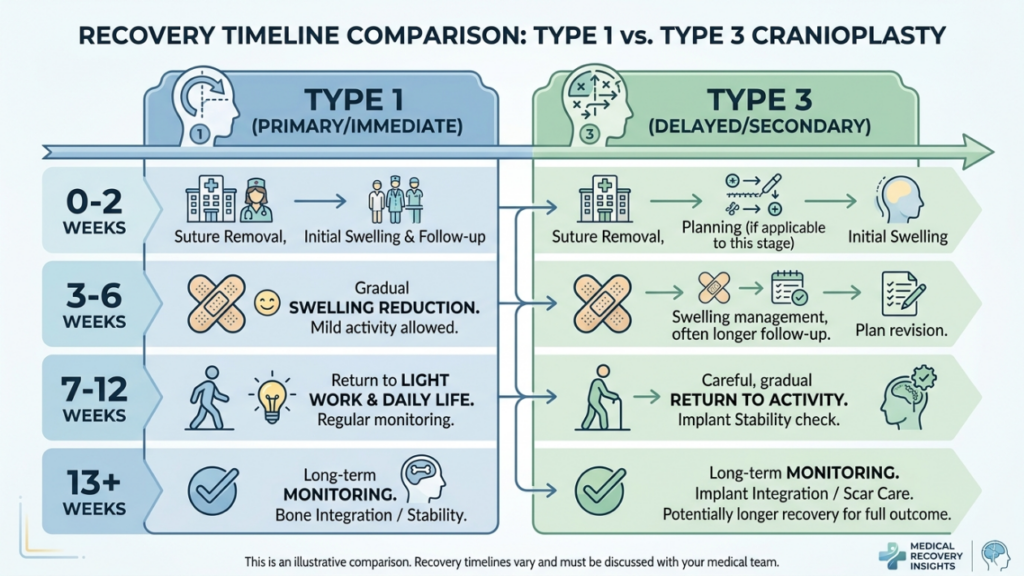
| I tempi di recupero | 1–2 settimane | 3-6 settimane |
| Risk of Complications | Basso | Da moderato ad alto |
| Costo | Inferiore | Più alto |
| Risultato estetico | Subtle contouring | Dramatic feminization |
Come i chirurghi decidono: tipo 1 vs. tipo 3
The choice between Type 1 and Type 3 cranioplasty depends on several factors, including the patient’s anatomical features, aesthetic goals, E surgical risks. Surgeons rely on a combination of clinical examination, Immagini 3D, E patient consultation to determine the most appropriate technique.
1. Valutazione anatomica
The first step is evaluating the patient’s frontal bone thickness E frontal sinus anatomy. UN CT scan O Ricostruzione 3D provides detailed insights into:
- Spessore osseo: Patients with thin frontal bones (less than 5 mm) are better suited for Type 1 cranioplasty, while those with thicker bones may require Type 3.
- Sinus Pneumatization: Extensive sinus pneumatization may necessitate Type 3 cranioplasty to avoid violating the sinus during burring.
- Degree of Bossing: Severe brow bossing often requires the dramatic reduction achievable only with Type 3 techniques.
2. Obiettivi estetici
Patients’ aesthetic expectations play a crucial role in technique selection. Those seeking subtle feminization may opt for Type 1 cranioplasty, while individuals with pronounced masculine features often require the transformative results of Type 3. Surgeons discuss realistic outcomes based on the patient’s anatomy and desired changes.
3. Rischi chirurgici e recupero
Type 3 cranioplasty carries higher risks, including sinus complications, cerebrospinal fluid leaks, E prolonged recovery. Surgeons assess the patient’s overall health, tolerance for surgery, and willingness to adhere to postoperative care. Patients with medical conditions that increase surgical risks may be advised to consider Type 1 or alternative procedures.
4. Pianificazione chirurgica virtuale (VSP)
Advancements in 3D virtual surgical planning have revolutionized cranioplasty. Surgeons use VSP to simulate osteotomies, setbacks, and outcomes, ensuring precision and minimizing risks. This technology is particularly valuable for Type 3 cranioplasty, where accurate bone repositioning is critical (3D Printing and Virtual Surgical Planning in Craniofacial and Orthognathic Surgery, 2025).
Cura e recupero postoperatorio
Recovery varies significantly between Type 1 and Type 3 cranioplasty. Understanding the postoperative process helps patients prepare for a smooth healing journey.
Recupero dopo cranioplastica di tipo 1
Patients undergoing Type 1 cranioplasty typically experience:
- Mild to Moderate Swelling: Resolves within 1–2 weeks.
- Minimal Discomfort: Managed with over-the-counter pain medications.
- Ritorno rapido alle attività: Most patients resume normal activities within 2 weeks.
Recupero dopo cranioplastica di tipo 3
Recovery from Type 3 cranioplasty is more involved due to the complexity of the procedure:
- Gonfiore e lividi significativi: May persist for 3–4 weeks.
- Moderate Pain: Prescription pain medications may be required for the first week.
- Ritorno graduale alle attività: Strenuous activities are restricted for 4–6 weeks.
- Visite di controllo: Regular monitoring to ensure proper healing and address any complications.
Both techniques require patients to avoid heavy lifting, esercizio fisico intenso, E direct pressure on the forehead during the initial recovery phase. Surgeons provide detailed postoperative instructions, including wound care, activity restrictions, and signs of complications to watch for.
Potenziali complicazioni e come evitarle
While cranioplasty is generally safe, complications can arise. Awareness of these risks and preventive measures is crucial for both surgeons and patients.
Complicazioni comuni
- Sinusite: Inflammation or infection of the frontal sinus, particularly in Type 3 cranioplasty if the sinus is violated.
- Perdita di liquido cerebrospinale (CSF): Rare but serious complication if the posterior table of the sinus is breached.
- Irregolarità del contorno: Over-thinning of bone in Type 1 or improper setback in Type 3 can lead to asymmetry or visible ridges.
- Formazione di mucocele: Blockage of sinus drainage pathways can result in mucus-filled cysts.
- Infezione: Risk is higher in Type 3 due to the longer operative time and use of implants.
Misure preventive
Surgeons employ several strategies to minimize complications:
- Pianificazione chirurgica precisa: 3D imaging and virtual surgical planning ensure accurate osteotomies and setbacks.
- Sinus Preservation: Avoiding violation of the frontal sinus during burring or osteotomy.
- Antibiotic Prophylaxis: Administered pre- and postoperatively to reduce infection risks.
- Monitoraggio postoperatorio: Regular follow-ups to detect early signs of complications.
- Educazione del paziente: Instructing patients on proper wound care, activity restrictions, and warning signs of complications.
Alternative alla cranioplastica di tipo 1 e di tipo 3
For patients who are not ideal candidates for Type 1 or Type 3 cranioplasty, alternative techniques may be considered:
- Innesto di grasso: Autologous fat transfer can soften forehead contours without altering bone structure. This is ideal for patients with mild irregularities or those seeking non-surgical options.
- Custom Implants: Pre-fabricated implants, such as PEEK (polyether ether ketone) O titanium, can be used to augment or reshape the forehead without osteotomy. These are particularly useful for patients with thin bones or sinus complications.
- Chirurgia ortognatica: In cases where rimodellamento della fronte is part of a broader facial feminization plan, orthognathic procedures (e.g., Le Fort I osteotomy) may be combined to address midface and jaw alignment.
- Endoscopic Techniques: Minimally invasive endoscopic approaches can reduce brow bossing with smaller incisions and faster recovery times.
Testimonianze dei pazienti e risultati concreti
Real-world outcomes provide valuable insights into the effectiveness and satisfaction rates of Type 1 and Type 3 cranioplasty. Patient testimonials highlight the transformative impact of these procedures:
Case Study 1: Type 1 Cranioplasty
A 28-year-old transgender woman sought subtle feminization of her forehead. With a thin frontal bone and minimal bossing, she opted for Type 1 cranioplasty. The procedure achieved a smoother contour with minimal downtime. She reported high satisfaction, noting that the results aligned with her expectations for a natural, feminine appearance.
Case Study 2: Type 3 Cranioplasty
A 35-year-old transgender woman presented with severe brow bossing and a thick frontal bone. Type 3 cranioplasty was performed, involving osteotomy and setback. The dramatic reduction in forehead projection significantly feminized her facial features. While recovery took longer, she expressed immense satisfaction with the results, stating that the procedure “changed her life.”
Case Study 3: Revision Surgery
A 40-year-old patient initially underwent Type 1 cranioplasty but was dissatisfied with the subtle results. She later opted for Type 3 cranioplasty to achieve more dramatic feminization. The revision surgery successfully addressed her concerns, demonstrating the importance of selecting the right technique based on anatomical needs and aesthetic goals.
Il ruolo della pianificazione chirurgica virtuale nella cranioplastica
Virtual surgical planning (VSP) has become a game-changer in cranioplasty, particularly for Type 3 procedures. VSP allows surgeons to:
- Simulate Osteotomies: Precisely plan bone cuts and repositioning to achieve optimal contouring.
- Predict Outcomes: Visualize postoperative results and adjust the surgical plan accordingly.
- Ridurre al minimo i rischi: Avoid critical structures such as the frontal sinus and supraorbital nerves.
- Enhance Communication: Share 3D models with patients to set realistic expectations and improve informed consent.
Studies have shown that VSP reduces operative time, improves accuracy, and enhances patient satisfaction (3D Printing and Virtual Surgical Planning in Craniofacial and Orthognathic Surgery, 2025). It is now considered the gold standard for complex cranioplasty procedures.

Domande frequenti
Qual è la principale differenza tra la cranioplastica di tipo 1 e quella di tipo 3?
La cranioplastica di tipo 1 prevede la limatura o la fresatura dello strato esterno dell'osso frontale per ridurne la prominenza, mentre la cranioplastica di tipo 3 richiede un'osteotomia (taglio osseo) e l'arretramento del segmento dell'osso frontale per ottenere un rimodellamento più marcato. Il tipo 1 è meno invasivo ed è indicato per prominenze lievi o moderate, mentre il tipo 3 è riservato a prominenze gravi o ossa frontali spesse.
Come fanno i chirurghi a decidere tra cranioplastica di tipo 1 e di tipo 3?
I chirurghi valutano lo spessore dell'osso frontale del paziente, il grado di prominenza delle sopracciglia e l'anatomia del seno frontale mediante tomografia computerizzata (TC) e immagini 3D. Il tipo 1 viene scelto per ossa più sottili e prominenza lieve, mentre il tipo 3 è preferibile per ossa più spesse, prominenza grave o pneumatizzazione estesa del seno. Anche gli obiettivi del paziente e la sua tolleranza ai rischi chirurgici influenzano la decisione.
Quali sono i rischi associati alla cranioplastica di tipo 3?
La cranioplastica di tipo 3 comporta rischi maggiori a causa della sua complessità, tra cui sinusite, perdite di liquido cerebrospinale, irregolarità del contorno, formazione di mucocele e infezioni. Questi rischi vengono minimizzati attraverso un'accurata pianificazione chirurgica, la preservazione dei seni paranasali e il monitoraggio postoperatorio. I pazienti vengono informati sui segnali di allarme e sulle cure di follow-up per garantire una pronta guarigione.
Quanto dura il periodo di recupero per una cranioplastica di tipo 1 rispetto a una di tipo 3?
Il recupero da una cranioplastica di tipo 1 richiede in genere 1-2 settimane, con lieve gonfiore e fastidio. La cranioplastica di tipo 3 richiede un recupero più lungo, da 3 a 6 settimane, a causa dell'intervento chirurgico più esteso e delle potenziali complicazioni. Si consiglia ai pazienti di evitare attività faticose e di seguire attentamente le istruzioni post-operatorie.
La cranioplastica di tipo 1 può ottenere gli stessi risultati della cranioplastica di tipo 3?
No, la cranioplastica di tipo 1 si limita a un rimodellamento sottile ed è ideale per bozze frontali da lievi a moderate. La cranioplastica di tipo 3 ottiene una femminilizzazione più marcata riposizionando il segmento osseo frontale, risultando quindi adatta a bozze frontali gravi o ossa frontali spesse. La scelta dipende dalle esigenze anatomiche e dagli obiettivi estetici della paziente.
Che ruolo svolge la pianificazione chirurgica virtuale nella cranioplastica?
La pianificazione chirurgica virtuale (VSP) consente ai chirurghi di simulare le osteotomie, prevedere i risultati e minimizzare i rischi evitando strutture critiche come il seno frontale. Migliora la precisione, riduce i tempi operatori e aumenta la soddisfazione del paziente fornendo una chiara visualizzazione del piano chirurgico e dei risultati attesi.
Esistono alternative non chirurgiche alla cranioplastica per la femminilizzazione della fronte?
Sì, tra le alternative non chirurgiche si annoverano il lipofilling per ammorbidire i contorni e gli impianti personalizzati (ad esempio, in PEEK o titanio) per rimodellare la fronte senza osteotomia. Queste opzioni sono ideali per pazienti con lievi irregolarità o per coloro che preferiscono evitare la chirurgia. Tuttavia, potrebbero non raggiungere lo stesso livello di femminilizzazione delle tecniche chirurgiche.
Cosa devo aspettarmi durante la visita per la ricostruzione della fronte?
Durante la visita, il chirurgo valuterà lo spessore dell'osso frontale, l'anatomia dei seni paranasali e il grado di prominenza ossea mediante esame clinico e immagini 3D. Discuterà i vostri obiettivi estetici, spiegherà le differenze tra cranioplastica di tipo 1 e di tipo 3 e vi consiglierà la tecnica più adatta in base alla vostra anatomia e alle vostre aspettative.