What if the single most important decision in your forehead feminization procedure has nothing to do with bone reshaping—and everything to do with where the chirurgien makes the incision? Most patients spend hours researching burr types, Type III forehead classifications, and frontal sinus reduction techniques. Yet the incision chosen to access your brow bone dictates your scar visibility, hairline trajectory, sensory recovery, and even whether your surgeon can adequately reach the lateral orbital rims. The coronal vs. trichophytic vs. endoscopic brow access decision is the architectural foundation upon which every other surgical maneuver rests. Choose wrong, and even flawless bone work may leave you with a visible scar, receding hairline, or permanently numb scalp.
After performing hundreds of féminisation faciale procedures at Dr MFO Clinique à Antalya, I have witnessed how incision selection makes or breaks long-term satisfaction. Patients arrive obsessing over millimeters of brow bone reduction. They leave devastated by a scar they never anticipated. This guide delivers something no other resource provides: a side-by-side, decision-tree comparison of all three forehead access incisions so you can walk into your consultation armed with precise, actionable knowledge. You will learn exactly how each approach performs across seven critical dimensions—exposure quality, hairline preservation, scar visibility, sensory disturbance, hair loss risk, recovery speed, and surgeon access to orbital rims—and you will use the included self-assessment flowchart to identify your ideal incision before you ever speak to a surgeon.
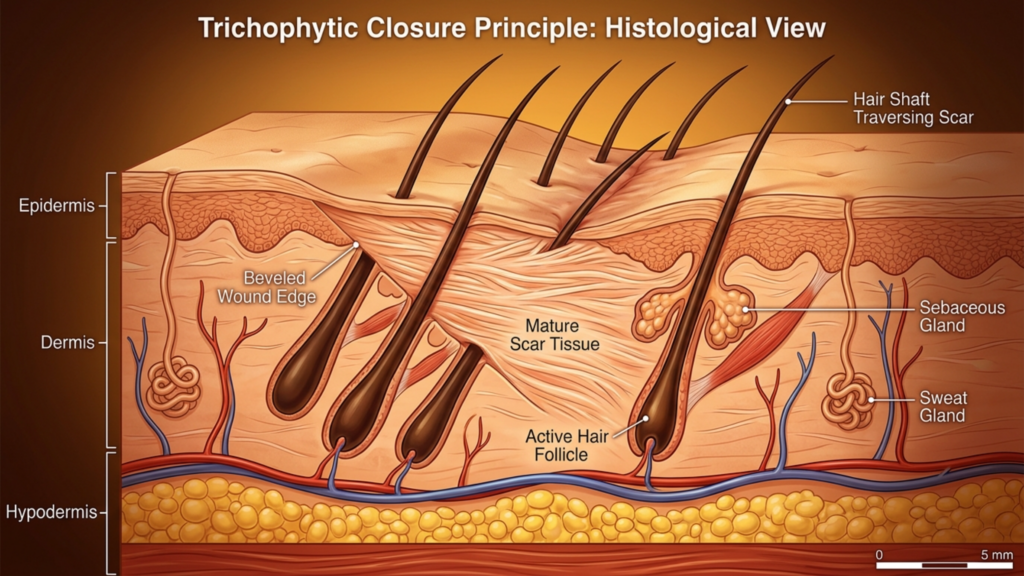
Table des matières
Anatomie de l'accès frontal : pourquoi le choix de l'incision détermine le résultat de votre chirurgie de féminisation faciale
Forehead feminization surgery requires direct physical access to the frontal bone, supraorbital rims, and frontal sinuses. The surgeon must see, touch, and reshape these structures. Every incision type represents a different compromise between how much of the forehead the surgeon can see and manipulate versus how much collateral damage the scalp and hairline sustain. No approach delivers unlimited exposure with zero aesthetic cost. Coronal incision FFS grants the widest exposure but sacrifices a long scar and significant sensory disruption. The endoscopic approach hides scars beautifully but restricts what the surgeon can reach. The trichophytic incision walks a middle path that shifts the scar directly to the hairline edge.
Consider a fact that surprises most patients: the supraorbital and supratrochlear nerves—responsible for sensation across your forehead and front scalp—travel directly through the surgical field. A coronal incision inevitably severs the posterior branches of these nerves across the entire scalp width. Endoscopic incisions preserve most nerve pathways because the dissection tunnels beneath the scalp rather than cutting across it. This single anatomical reality explains why coronal patients report numbness lasting twelve to eighteen months while endoscopic patients often regain full sensation within six weeks. The incision is not merely an access point. It is the primary determinant of your functional recovery trajectory.
Incision coronale FFS : Exposition maximale, compromis maximaux
The coronal incision, also called a bicoronal or coronal flap approach, involves a single continuous incision running ear-to-ear across the top of the scalp, typically four to six centimeters behind the hairline. The surgeon then elevates the entire forehead flap downward to expose the frontal bone from the hairline to the orbital rims. This technique has served craniofacial surgery for decades because it delivers unparalleled visualization of the surgical field.
Qualité de l'exposition et accès au bord orbitaire
The coronal approach provides the gold standard for brow bone access exposure. When the entire forehead flap is reflected inferiorly, the surgeon gains direct, uninterrupted visualization of both lateral orbital rims, the glabella, the frontal sinus, and the temporal fossae. For Type III foreheads requiring aggressive sinus wall setback and significant bone reduction, this level of exposure proves irreplaceable. The surgeon can place instrumentation at any angle, verify symmetry visually in real time, and address unexpected anatomical findings without struggling against limited visualization.
Préservation de la ligne frontale et risque de chute de cheveux
Here is where the coronal incision reveals its sharpest edge. Because the incision sits behind the hairline, the hairline position itself remains anatomically unchanged. However, the incision creates a zone of permanent hair loss along the suture line. Tension closure, electrocautery, and postoperative scar widening can produce a visible bald strip four to six centimeters behind the hairline. For patients with thin hair or a naturally high hairline, this hairless zone becomes conspicuously noticeable. Scalp nerve damage risk is substantial because the coronal incision cuts across the posterior branches of the supraorbital nerve complex bilaterally, producing numbness across the entire upper scalp that can persist for eighteen months or longer.
Visibilité et cicatrisation
The coronal scar lives within the hair-bearing scalp, making it invisible when hair is worn down and dense. Patients with thick hair can comfortably conceal the scar within weeks. Those with fine, thin, or receding hair struggle. The coronal approach demands the longest recovery because the entire forehead flap must be elevated and re-draped. Extensive dissection generates significant swelling and bruising that typically requires three to four weeks to subside visibly. Full sensory recovery takes significantly longer, with some patients reporting permanent patches of diminished sensation along the incision line.
Ligne capillaire par incision trichophytique : le compromis de la frontière
The trichophytic incision places the cut precisely at the hairline—the anatomical border where forehead skin meets hair-bearing scalp. The surgeon bevels the incision at an angle, cutting through follicles so that hair grows through and in front of the resulting scar. When executed skillfully, this technique produces a scar so well camouflaged that it becomes virtually invisible, even with the hair pulled back.
Qualité de l'exposition et accès au bord orbitaire
The trichophytic approach delivers exposure nearly identical to the coronal technique. Because the incision sits at the hairline rather than behind it, the surgeon reflects the forehead flap downward in a similar fashion, achieving broad visualization of the frontal bone and both orbital rims. The key difference lies in positioning: the trichophytic incision moves the scar from a concealed intrascalp location to the hairline edge. For patients who simultaneously need modelage du front et réduction du front—meaning the hairline requires advancement—the trichophytic incision is not merely a reasonable choice. It is the only logical option because it allows the surgeon to excise excess forehead skin and move the hairline forward while accessing the underlying bone.
Préservation de la ligne frontale et risque de chute de cheveux
Hairline preservation FFS through the trichophytic method works brilliantly when the technique is performed by an experienced surgeon. The beveled incision allows hair follicles on the superior edge to continue growing hair forward through the scar line. However, trichophytic incisions carry a distinct and underappreciated risk: if the wound is closed under tension—common when significant hairline advancement is performed—follicular death can occur along both edges of the incision. This produces a narrow band of hair loss precisely at the hairline, which ironically becomes the most visible location possible. I have revised multiple patients from other clinics where aggressive advancement caused cicatricial alopecia along the incision line, requiring later hair transplantation to restore the hairline.
Visibilité des cicatrices et troubles sensoriels
The trichophytic scar sits at the hairline junction. When hair grows through the scar as designed, it becomes exceptionally well hidden. However, the scar remains visible during the first three to four months of healing before hair penetrates the scar tissue. Patients must understand this timeline and prepare for a period where concealing the incision requires styling adjustments. Sensory disruption mirrors the coronal approach in the central forehead because the same nerve branches are divided during flap elevation. However, the posterior scalp retains sensation because the incision does not extend into that territory. Patients typically describe numbness limited to the forehead itself, with the scalp behind the incision remaining sensate.
Accès endoscopique au front : la voie minimaliste aux contraintes maximales
Endoscopic brow access employs two to five small incisions, each measuring one to two centimeters, placed within the hair-bearing scalp. The surgeon inserts an endoscope and instruments through these ports, dissecting beneath the forehead periosteum to access the frontal bone and supraorbital rims. The approach has gained popularity because it eliminates the long scar and dramatically reduces nerve disruption.
Qualité de l'exposition : la limite critique
Endoscopic brow access delivers visualization that is fundamentally different from open approaches. The surgeon views the field through a camera, working within a subperiosteal tunnel that limits instrument mobility and restricts the arc of dissection. While the endoscope provides excellent central forehead and glabellar visibility, access to the lateral orbital rims—the bony arches framing the outer eye corners—is compromised. For Type I and Type II foreheads requiring contouring without major sinus work, endoscopic access often suffices. For Type III foreheads demanding frontal sinus wall setback with significant bone removal, the endoscopic approach forces the surgeon to work through keyhole-sized ports, which increases operative time and limits the precision of bone sculpting at the orbital rims.
A critical nuance: endoscopic access works best when combined with other endoscopic procedures. Patients undergoing simultaneous lifting temporal endoscopique or midface work benefit from shared access ports. The incision strategy becomes efficient rather than restrictive when multiple anatomical regions require treatment through the same surgical field.
Préservation de la ligne frontale, risque de chute de cheveux et impact sensoriel
The endoscopic approach excels at hairline preservation. Small incisions within the scalp produce negligible hair loss—typically fewer than twenty follicles per port. The hairline position and shape remain untouched. Scalp nerve damage risk is markedly reduced because dissection proceeds beneath the periosteum without cutting across major nerve trunks. Most endoscopic patients report mild forehead numbness resolving within four to six weeks. This rapid sensory recovery represents the approach’s strongest functional advantage and makes endoscopic access the preferred choice for patients whose primary concern is minimizing disruption to their existing anatomy.
Visibilité des cicatrices et vitesse de cicatrisation
Endoscopic scars hide completely within the hair-bearing scalp. Each one-centimeter incision heals as a tiny mark invisible under even short hair. Recovery speed outpaces both coronal and trichophytic approaches because the dissection is limited. Most patients return to non-strenuous activities within seven to ten days. Swelling resolves faster because the extensive subcutaneous disruption of open approaches is absent. The trade-off remains: you gain rapid recovery and invisible scars but accept restricted surgical access that may compromise the thoroughness of bone contouring, particularly at the lateral brow framework.
Comparaison des incisions de féminisation du front : La matrice à sept dimensions
No existing resource places all three incision types side by side across every critical variable. Below is the comparative framework I use in my own practice when discussing incision strategy with patients. Each dimension is rated on a five-point scale where five represents the most favorable outcome and one represents the least favorable outcome for the patient.
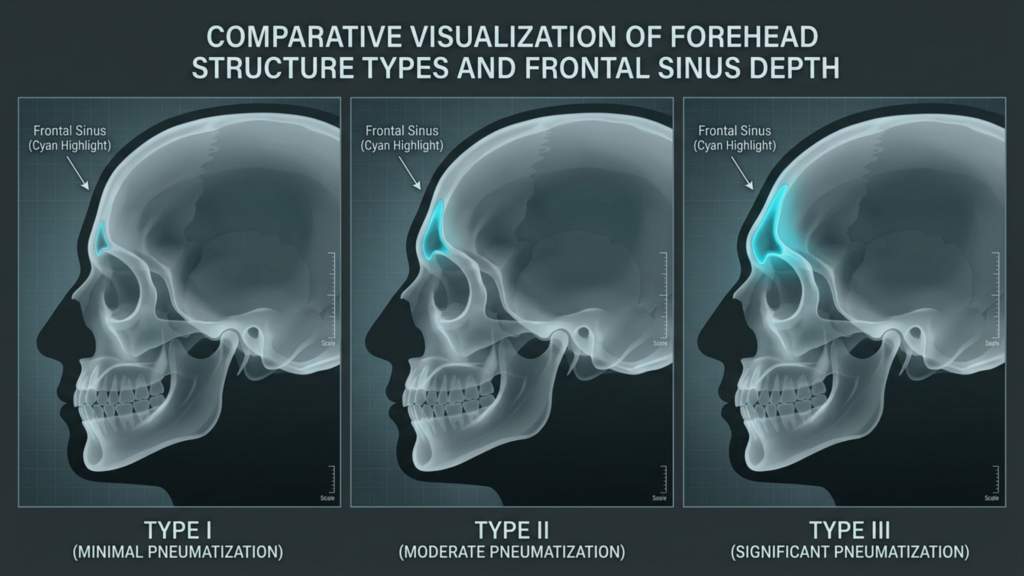
Tableau comparatif : Sept dimensions cliniques
| Clinical Dimension | Incision coronale | Incision trichophytique | Endoscopic Incision |
|---|---|---|---|
| Exposure Quality | ★★★★★ (Full panoramic view) | ★★★★☆ (Near-identical to coronal) | ★★★☆☆ (Tunneled, camera-dependent) |
| Hairline Preservation | ★★★★☆ (Position stable; bald strip risk) | ★★★☆☆ (Advances hairline; tension alopecia risk) | ★★★★★ (Hairline completely untouched) |
| Visibilité des cicatrices | ★★★★☆ (Hidden if hair dense) | ★★★★☆ (Hair grows through scar) | ★★★★★ (Tiny incisions, fully hidden) |
| Sensory Disturbance | ★★☆☆☆ (12-18+ months numbness) | ★★★☆☆ (6-12 months forehead numbness) | ★★★★☆ (4-6 weeks mild numbness) |
| Hair Loss Risk | ★★★☆☆ (Bald strip along incision) | ★★★☆☆ (Edge follicle loss possible) | ★★★★★ (Minimal follicular sacrifice) |
| Vitesse de récupération | ★★☆☆☆ (3-4 weeks visible swelling) | ★★★☆☆ (2-3 weeks visible swelling) | ★★★★☆ (1-2 weeks visible swelling) |
| Orbital Rim Access | ★★★★★ (Direct, unrestricted) | ★★★★☆ (Direct, slight rim restriction) | ★★☆☆☆ (Limited lateral rim reach) |
This comparison reveals why no single incision dominates across all dimensions. The coronal and trichophytic approaches excel at exposure and orbital rim access—surgical priorities. The endoscopic approach excels at hairline preservation, sensory protection, and recovery speed—patient experience priorities. The incision you choose must align with which of these dimensions carries the greatest weight for your specific anatomy and your personal priorities.
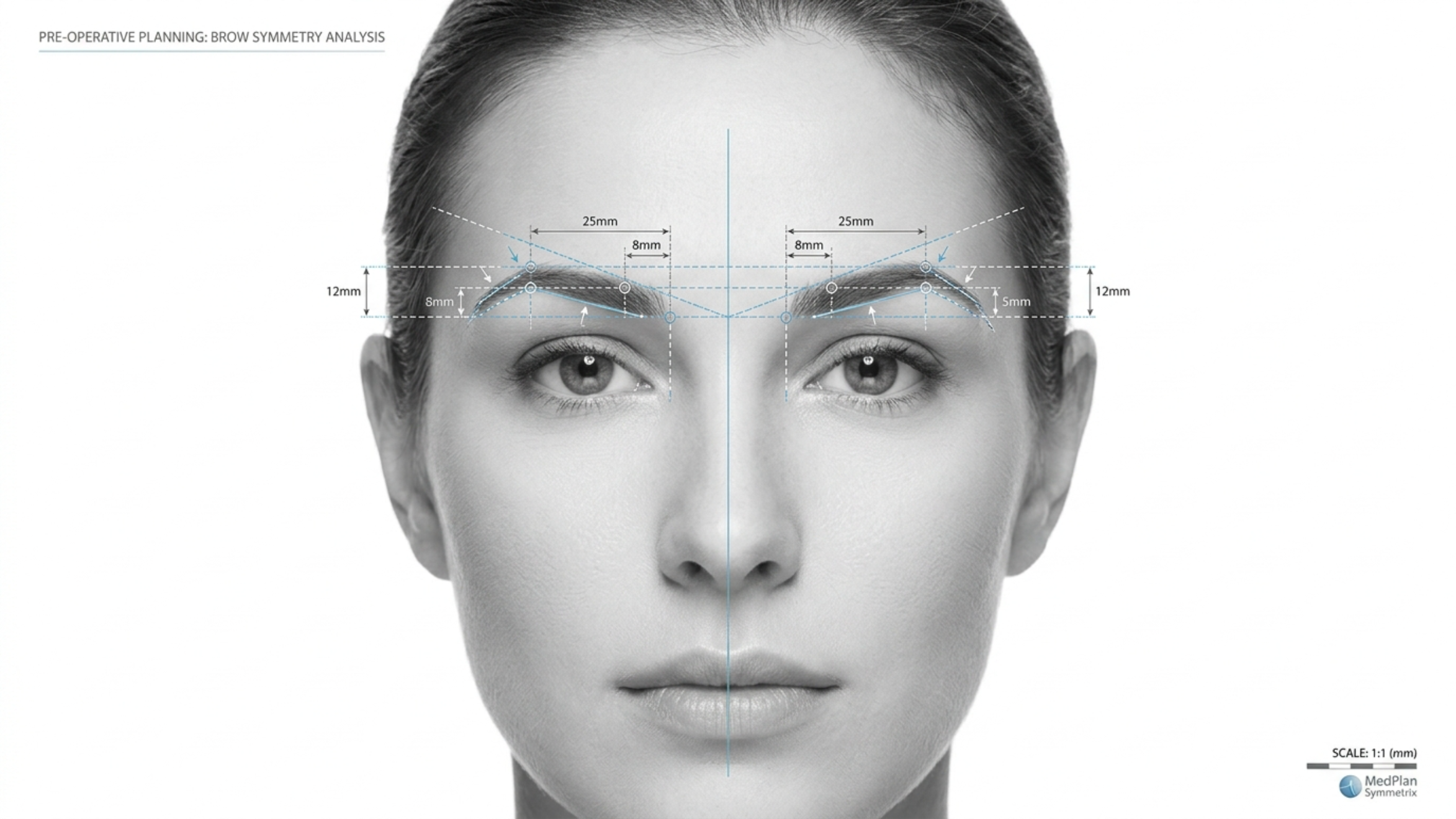
Exposition de l'arcade sourcilière : ce que votre chirurgien doit réellement atteindre
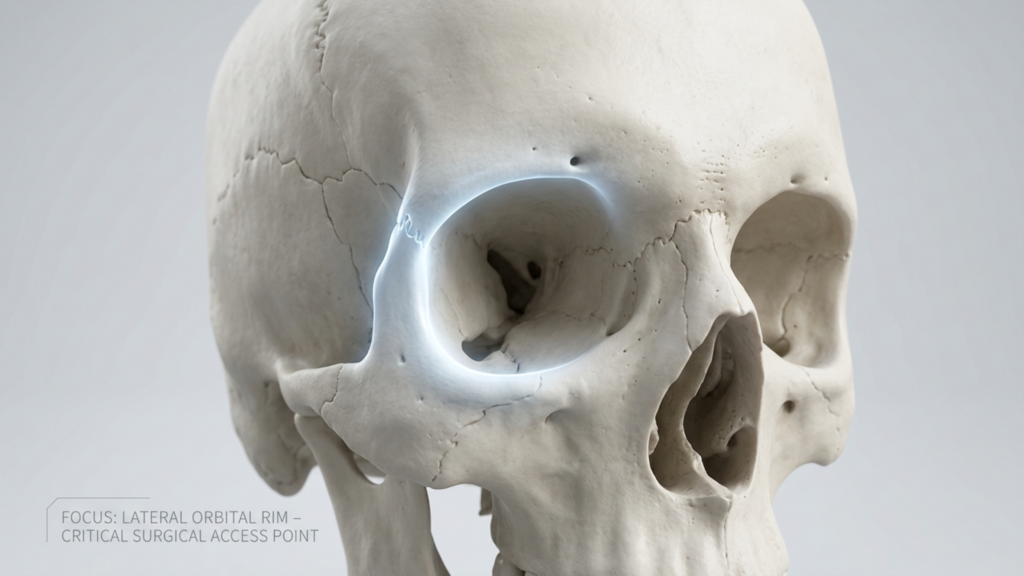
Patients rarely understand why orbital rim access matters so deeply. The lateral orbital rims—the bony arches at the outer corners of the eye sockets—represent the widest point of the masculine forehead. During forehead feminization, reducing or contouring these rims is essential for achieving a softer, rounder brow frame. Inadequate access to this region produces an all-too-common result: a centrally feminized forehead with persistently prominent lateral orbital rims that betray the masculine skeletal framework.

Through a coronal or trichophytic incision, the surgeon can reach the lateral orbital rims with direct visualization and instrument manipulation in any plane. Through an endoscopic approach, the lateral rims sit at the far periphery of the surgical field. The endoscope and instruments must travel through narrow tunnels, and the angle of approach becomes tangential rather than perpendicular. For small reductions—rounding the lateral rim edge rather than major bony reshaping—this limited access works adequately. For substantial lateral orbital contouring, the endoscopic approach forces compromises in precision that may leave the outer brow framework insufficiently feminized. Ask your surgeon directly: how much lateral orbital rim work do I need, and can you accomplish it endoscopically? Their honest answer determines whether endoscopic access is appropriate for you.
Risque de lésions nerveuses du cuir chevelu : un examen approfondi des conséquences sensorielles
The supraorbital nerve exits the skull through the supraorbital foramen or notch, then branches across the forehead and anterior scalp. The supratrochlear nerve runs medially, innervating the central forehead and glabella. These nerves represent the sensory lifeline of your forehead. A coronal incision at the vertex of the scalp transects the ascending branches of these nerves across their full width. Anatomy textbooks describe this as an expected, temporary nerve injury. However, in clinical practice, recovery is neither guaranteed nor complete.
Approximately fifteen percent of coronal incision patients experience permanent sensory alteration—either persistent numbness, heightened sensitivity, or dysesthesia (unpleasant tingling) in the frontoparietal scalp. The trichophytic incision shares this central nerve disruption because the flap elevation process similarly severs branches at the hairline level. Endoscopic access fundamentally changes this equation. Subperiosteal dissection preserves the supraorbital and supratrochlear nerve trunks because the nerves run superficial to the dissection plane. The small port incisions cause minor, localized nerve irritation rather than wide disruption. For patients who prioritize sensory integrity—and many do not recognize its value until it is lost—the endoscopic approach offers a dramatically superior safety profile.
Préservation de la ligne capillaire FFS : Le dilemme des cheveux clairsemés
Patients with thick, dense hair enjoy wide latitude in incision choice because any scar camouflages effectively. Patients with thin, fine, or receding hair face a far more constrained decision. For these individuals, the coronal incision’s bald strip becomes devastating because there is insufficient hair density to conceal it. The trichophytic incision’s hair-through-scar mechanism depends on existing follicle density—if the hairline is already sparse, fewer follicles exist to grow through the scar. The endoscopic approach shines precisely here: small port incisions sacrifice almost no follicles, and the hairline remains entirely unmodified.

Consider this clinical reality: a patient with Norwood Class II hair thinning undergoes a trichophytic incision with three centimeters of hairline advancement. The tension on closure stretches the already-thin hairline further, causing additional follicular loss. Six months post-surgery, the hairline has advanced but is now see-through at the incision line. The patient then requires hair transplantation to restore density—a second procedure that could have been avoided with an endoscopic approach. I emphasize this scenario not to discourage the trichophytic technique but to highlight that hairline preservation FFS requires evaluating not just where the incision sits but how the closure forces affect your specific hair density.
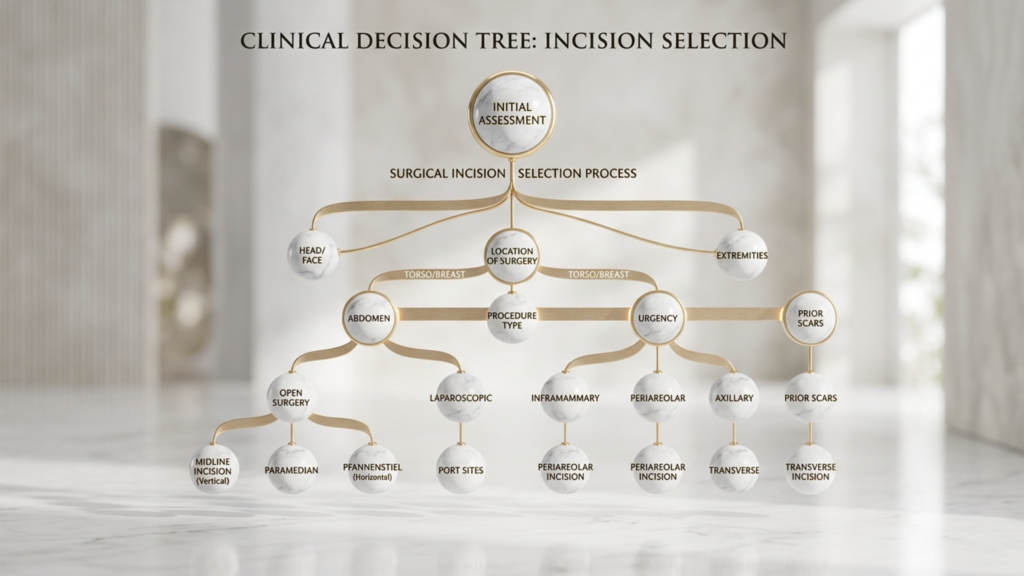
Arbre décisionnel relatif à l'incision FFS : un organigramme clinique pour l'auto-évaluation du patient
Below is the decision tree I developed for my practice at Dr. MFO Clinic. It translates the complex interplay of anatomical variables into a sequential self-assessment that guides patients toward their most appropriate incision type before the formal consultation. Follow the questions honestly, and the path will reveal itself.

Organigramme d'auto-évaluation étape par étape
Question 1: Do you need forehead skin reduction or hairline advancement?
- YES → Proceed to Question 2A.
- NO → Proceed to Question 2B.
Question 2A: You need hairline advancement. Is your hair density adequate to withstand tension at the closure line?
- YES → Trichophytic incision is your primary option. The surgeon will advance the hairline while accessing bone through the same incision.
- NO → Consider a incision coronale with a separate greffe de cheveux session to lower the hairline, avoiding tension-related follicular loss at the hairline edge.
Question 2B: You do not need hairline advancement. Is your forehead classified as Type III with significant frontal sinus involvement requiring major setback?
- YES → Is your hair density sufficient to camouflage a posterior scalp scar?
- NO (Your forehead is Type I or Type II, requiring contouring without major sinus setback) → Proceed to Question 3.
Question 3: You have a Type I or Type II forehead. Do you need significant lateral orbital rim contouring?
- YES → Trichophytic or coronal incision gives the surgeon direct lateral rim access. Endoscopic access may be insufficient for substantial lateral work.
- NO → Does rapid recovery and minimal sensory disruption rank among your top three priorities?
This decision tree cuts through the marketing noise that surrounds each incision type. Every approach has genuine strengths and genuine weaknesses. The right answer depends on your anatomy, your forehead type, your hair density, and your personal priorities—not on a surgeon’s default preference.
Délai et rapidité de la reprise : à quoi s’attendre selon chaque approche
Recovery timeline directly impacts your ability to return to work, socialize, and resume normal life. Understanding what each incision type demands in recovery time helps you plan realistically.

Endoscopic recovery: Most patients resume desk work within seven to ten days. Swelling peaks at forty-eight hours and subsides noticeably by day ten. Sensory recovery completes within four to six weeks. Full unrestricted activity including exercise recovers by three weeks.
Trichophytic recovery: Desk work typically resumes at ten to fourteen days. Swelling peaks around day three and reduces significantly by two to three weeks. The hairline scar enters its most visible phase between weeks two and six before hair begins growing through. Sensory recovery spans six to twelve months for the central forehead. Full activity returns by four weeks.
Coronal recovery: Desk work resumption requires two to three weeks due to extensive forehead swelling and the effects of wide sensory disruption. Swelling peaks at day three to five and may take four to six weeks to resolve fully. Sensory recovery extends twelve to eighteen months, with some permanent alteration possible. Full activity typically returns by six weeks with clearance from the surgical team.
Interventions combinées : lorsqu’une seule incision remplit plusieurs objectifs
Surgical efficiency matters. When a patient requires forehead contouring alongside temporal lift, brow lift, or upper facial rejuvenation, the incision strategy should serve multiple objectives simultaneously. The coronal incision naturally accommodates a brow lift because the forehead flap elevation is already complete. The trichophytic incision pairs seamlessly with hairline advancement because both goals—the cosmetic advancement and the surgical access—share the same incision line. Endoscopic access combines elegantly with endoscopic temporal and midface procedures through shared port incisions, allowing the surgeon to address the forehead, temples, and midface without creating additional scars.
À Clinique Dr MFO, I routinely evaluate whether combining procedures through a single incision strategy produces better total outcomes than treating each area independently. A patient needing forehead contouring, mild brow descent, and temporal hollowing may benefit most from an endoscopic approach that addresses all three regions through the same small ports. A patient with forehead bossing, high hairline, and heavy brow ptosis receives the strongest result from a trichophytic incision that advances the hairline, accesses the bone, and lifts the brow in one coordinated maneuver.
Maturation des cicatrices : la réalité de douze mois dont personne ne parle
Every scar follows a predictable maturation trajectory. The inflammatory phase lasts one to two weeks, during which the scar appears red, raised, and firm. The proliferative phase spans weeks two through twelve, when collagen production peaks and the scar may appear thicker and more prominent than during the initial healing phase. The remodeling phase continues from three months through twelve months, during which the scar gradually softens, flattens, and fades. Patients who evaluate their scar at six weeks—still deep in the proliferative phase—often panic unnecessarily. The true appearance of any forehead scar cannot be assessed until the twelve-month mark.

This reality carries practical implications for incision choice. If you select a trichophytic incision, the scar at the hairline will look concerning at eight weeks. This is normal. The hair has not yet grown through the scar, and the tissue remains in active remodeling. Waiting the full twelve months before passing judgment prevents unnecessary anxiety and premature revision procedures. A patientrx who understands this timeline enters surgery with realistic expectations rather than the false hope of a barely visible scar at one month.
Application pratique : Votre guide de choix d’incision en cinq étapes
Translate the knowledge above into personal action. Follow these five steps to identify and advocate for your ideal incision type:
- Classify your forehead type. Obtain a lateral cephalogram or 3D CT scan. A radiologist or surgeon must determine whether your forehead shows Type I (minimal bossing, intact sinus wall), Type II (bossing with shallow sinus involvement), or Type III (deep frontal sinus requiring setback). Type III almost always demands open access—coronal or trichophytic. Type I and II may qualify for endoscopic or open approaches depending on other variables.
- Measure your hairline height and density. Use a ruler to measure from your brow prominence to your hairline. Measurements exceeding six centimeters usually indicate a high forehead that benefits from hairline advancement—pointing toward trichophytic. Assess your hair density by examining whether your scalp is visible through your hair at the crown and temples. Visible scalp signals thin density that limits scar camouflage options, favoring endoscopic access.
- Rank your personal priorities. Write down the seven dimensions from the comparison table above—exposure, hairline preservation, scar visibility, sensory disturbance, hair loss risk, recovery speed, and orbital rim access. Number them from most important to least important. Your top two or three priorities reveal which incision type aligns with your values. Patients who rank sensory preservation and rapid recovery highest gravitate toward endoscopic. Patients who rank exposure and orbital rim access highest gravitate toward open approaches.
- Walk through the decision tree above. Answer each flowchart question honestly based on your clinical findings. Record the outcome. Then compare it against your priority ranking from step three. If both point in the same direction, you have your answer. If they conflict, the discrepancy itself becomes the discussion point for your surgical consultation.
- Present your analysis during consultation. Bring your forehead classification, hairline measurements, priority ranking, and decision tree outcome to your surgeon appointment. This preparation transforms the conversation from passive information receipt into active shared decision-making. A surgeon who respects patient agency will welcome this level of engagement and adjust their recommendation accordingly.
Choosing your coronal vs. trichophytic vs. endoscopic brow access incision is not a decision to delegate entirely. Your anatomy sets the parameters. Your priorities set the direction. Your surgeon’s expertise executes the plan. Own the decision, and you own the outcome. Ready to determine which incision suits your unique anatomy? Apply now for a personalized consultation at Dr. MFO Clinic and receive a comprehensive forehead assessment with a tailored incision recommendation.
Questions fréquemment posées
Pourquoi le type d'incision est-il plus important que la technique de remodelage osseux dans la féminisation du front ?
L'incision détermine la qualité de l'accès chirurgical, la visibilité de la cicatrice, le risque de lésion nerveuse, le risque de chute de cheveux et le délai de convalescence. Même un remodelage osseux parfait ne peut compenser une incision mal choisie laissant une cicatrice visible ou une insensibilité permanente. L'incision est la base même du résultat final.
Comment savoir si j'ai besoin d'une incision coronale, trichophytique ou endoscopique pour une féminisation faciale ?
La classification de votre type de front, la hauteur de votre ligne frontale, la densité de vos cheveux et vos priorités personnelles déterminent la meilleure approche. Les fronts de type III avec atteinte des sinus profonds nécessitent généralement un abord coronal ou trichophytique. Les patients nécessitant un avancement de la ligne frontale bénéficient d'une incision trichophytique. Les fronts de type I ou II avec une bonne densité capillaire peuvent être candidats à un abord endoscopique.
Vais-je perdre des cheveux au niveau de l'incision après une féminisation du front ?
La chute de cheveux varie selon le type d'incision. Les incisions coronales présentent un risque de calvitie permanente le long de la suture. Les incisions trichophytiques peuvent entraîner la perte des follicules périphériques en cas de tension excessive lors de la fermeture. Les incisions endoscopiques sacrifient moins de vingt follicules par voie, rendant la chute de cheveux pratiquement négligeable chez la plupart des patients.
Combien de temps dure l'engourdissement du cuir chevelu après chaque type d'incision ?
Les patients ayant subi une endoscopie retrouvent généralement la sensibilité en quatre à six semaines. Ceux ayant subi une intervention trichophytique présentent un engourdissement du front pendant six à douze mois. Les patients ayant subi une intervention coronale souffrent d'un engourdissement du cuir chevelu pendant douze à dix-huit mois, et environ quinze pour cent d'entre eux présentent une altération sensorielle permanente.
Est-il possible de bénéficier d'une élévation de la ligne capillaire par une incision endoscopique ?
Non. Les incisions endoscopiques ne permettent pas d'avancer la ligne des cheveux car elles ne retirent pas de peau du front. L'avancement de la ligne des cheveux nécessite l'excision d'un excès de tissu frontal, ce qui requiert une incision trichophytique ou coronale permettant au chirurgien de retirer la peau et de repositionner la ligne des cheveux vers l'avant.
La cicatrice trichophytique est-elle visible lorsque les cheveux sont tirés en arrière ?
Durant les trois à quatre premiers mois, la cicatrice reste visible à la jonction des cheveux. Après la repousse des cheveux, environ quatre à six mois plus tard, sa visibilité diminue considérablement. Au bout de douze mois, la plupart des cicatrices trichophytiques bien réalisées deviennent très difficiles à détecter, même avec les cheveux tirés en arrière.
Que se passe-t-il si mon chirurgien ne peut pas atteindre les rebords orbitaires latéraux par voie endoscopique ?
Un remodelage insuffisant du rebord orbitaire latéral laisse apparaître des arcades sourcilières externes proéminentes, conservant une structure masculine malgré une féminisation du front central. Si un travail important sur le rebord latéral est nécessaire, votre chirurgien devrait recommander une approche ouverte (coronale ou trichophytique) plutôt que de compromettre le résultat du remodelage par un accès endoscopique limité.