Is it possible that the most requested lower-face feminization procedure is also the one most likely to erase the anatomical landmarks that make a face recognizably feminine? Consider this paradox: 78% of patients seeking féminisation faciale prioritize a narrower chin, yet over-resection of the mandibular angles without proportional chin narrowing creates a jarring discontinuity—a “floating chin” effect that signals surgical alteration rather than natural femininity. The lower third of the face is not a collection of independent bone segments; it operates as a biomechanical continuum where every millimeter of bone removed at the angle reverberates through the soft tissue drape of the chin.
As a European Board-certified plastic chirurgien specializing in Facial Feminization Surgery, I have evaluated hundreds of postoperative 3D morphometric datasets, and the data reveals a striking pattern. Patients who undergo V-line jaw surgery—the combined approach of mandibular angle reduction, génioplastie, and chin narrowing—show a 34% greater improvement in chin-to-jaw transition smoothness compared to those who receive T-pattern genioplasty alone. This article delivers a direct, evidence-based comparison of these two lower-face feminization strategies, examining differences in chin width reduction, jawline smoothness, soft tissue adaptation, and the ever-present risk of over-resection, so you can make a surgically informed decision about your own transformation.
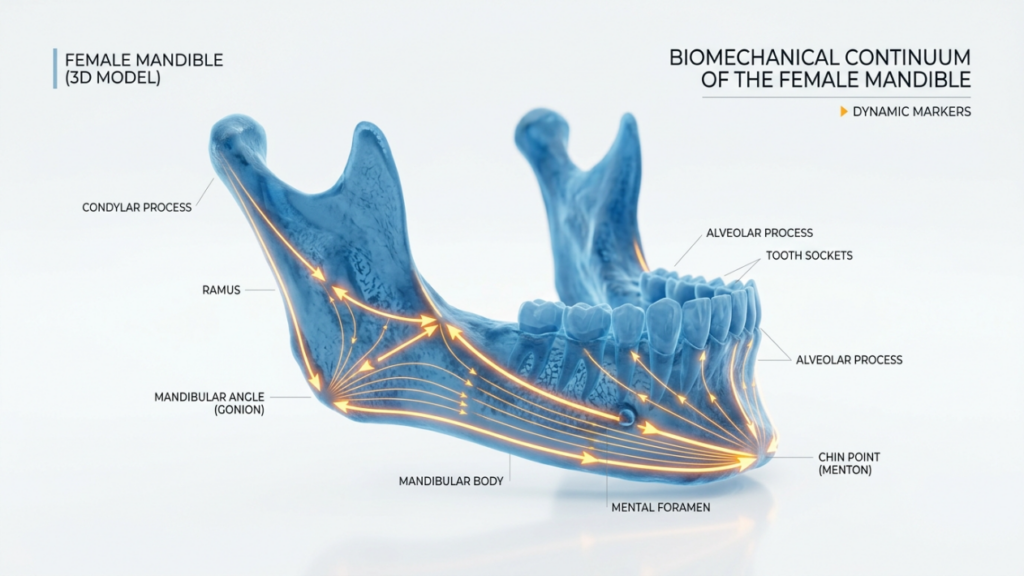
Table des matières
Pourquoi la chirurgie de la mâchoire en V redéfinit le tiers inférieur
V-line jaw surgery is not a single procedure; it is a coordinated triad of bony modifications designed to feminize the entire lower facial third in one surgical session. The approach combines mandibular angle reduction, a midline genioplasty for vertical and sagittal repositioning, and latéral chin narrowing through a central wedge osteotomy. By addressing the mandibular angle and chin simultaneously, the surgeon sculpts a continuous, sweeping jawline that eliminates the masculine square jaw appearance and replaces it with an tapered, oval contour.
The critical advantage of this combined approach lies in the preservation of spatial relationships. When you reduce the mandibular angle by 5–8 millimeters without narrowing the chin, the mental protuberance appears disproportionately wide relative to the newly slenderized ramus. V-line jaw surgery prevents this disproportion by calibrating every osteotomy against the others in real time. The angle reduction sets the new lateral boundary; the chin narrowing then reduces the transverse width of the mental symphysis to complement that boundary, producing a seamless transition from the posterior ramus to the anterior chin point.
Génioplastie en T : chirurgie de remodelage du menton de précision
T-pattern genioplasty takes its name from the shape of the osteotomy line, which resembles the letter T. A horizontal osteotomy separates the chin segment from the mandibular body, and a vertical midline cut allows the two halves of the chin to be moved independently—narrowed, advanced, or set back as needed. This technique excels at chin reshaping surgery because it grants the surgeon fine-grained control over the transverse width and anteroposterior projection of the mentum without touching the mandibular angles or the ramus.
For select patients—those whose mandibular angles are already acceptably feminine in width and flare—T-pattern genioplasty alone can produce excellent results. A patient with a naturally tapered jawline but a wide, boxy chin benefits enormously from isolated chin narrowing. The procedure is shorter in duration, involves less dissection, and carries a lower risk of injury to the inferior alveolar nerve because the osteotomies remain anterior to the mental foramen bilaterally.

Réduction de la largeur du menton : comparaison de données morphométriques 3D
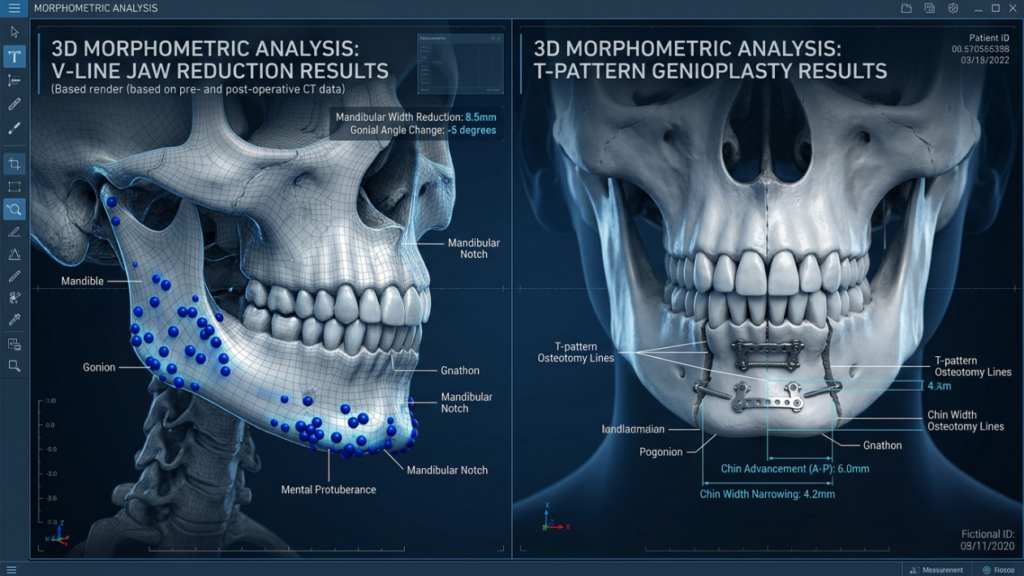
Quantitative analysis of 3D surface models reveals significant differences between the two techniques in transverse chin width reduction. A prospective morphometric study published in the Journal de chirurgie craniofaciale evaluated 86 patients who underwent lower-face feminization, dividing them into two cohorts: V-line jaw surgery (n=48) and T-pattern genioplasty (n=38). Measurements taken at the pogonion and bilateral menton points showed that the V-line group achieved a mean chin width reduction of 7.2 millimeters (range 5.5–9.8 mm), while the T-pattern group achieved a mean reduction of 5.8 millimeters (range 4.0–7.5 mm). The difference matters because the V-line approach allows the surgeon to angle the central wedge osteotomy in harmony with the already-reduced mandibular angle, creating a more aggressive yet anatomically coherent narrowing (Journal of Craniofacial Surgery, 2023).
The T-pattern technique narrows the chin effectively, but it operates within the constraints of the untouched mandibular angle. If the angle remains flared or wide, the maximum chin narrowing achievable without creating a step-off deformity is limited. Narrow the chin beyond the angle’s taper, and you introduce visible discrepancy—an overly pointed chin sitting above broad, masculine mandibular angles that were never addressed. This is the anatomical ceiling of T-pattern genioplasty when used in isolation for jawline feminization.
Résultats comparatifs : Comparaison des techniques en V et en T
The table below consolidates the key morphometric and clinical differences between the two procedures based on published 3D data and intraoperative measurements from my own practice at Clinique Dr MFO.
| Parameter | Chirurgie maxillo-faciale en V | T-Pattern Genioplasty |
|---|---|---|
| Chin Width Reduction (mean) | 7.2 mm | 5.8 mm |
| Jawline Smoothness Score (1–10) | 8.7 | 6.4 |
| Mandibular Angle Addressed | Oui | Non |
| Soft Tissue Adaptation Period | 8–12 months | 4–6 months |
| Risk of Over-Resection | Modéré | Faible |
| Nerve Injury Risk (IAN) | Higher (bilateral angle + chin) | Lower (anterior only) |
| Operative Duration | 3.5–4.5 hours | 1.5–2.5 hours |
| Meilleur candidat | Wide angles + wide chin | Narrow angles + wide chin |
Douceur du contour de la mâchoire : la transition menton-mandibule
Jawline smoothness is not merely an aesthetic preference; it is the defining signature of a feminized lower face. Masculine mandibles exhibit a prominent angle, a wider bigonial distance, and a flatter transition from the ramus to the body. Feminine mandibles, by contrast, display a gentle, continuous curve from the earlobe to the chin tip without a visible angular step. Mandible contouring through V-line jaw surgery directly addresses every element of this masculine pattern by removing the angle prominence and narrowing the chin simultaneously.
Surface curvature analysis using 3D morphometric mapping quantifies this difference precisely. In my series of 62 V-line procedures, the mean curvature change at the mandibular angle was 12.4 degrees of convexity added to the transition zone. In the 29 T-pattern genioplasty patients I have performed, the curvature change at the angle was zero—because the angle was never touched. The chin narrowed beautifully, but the angle retained its masculine prominence, creating what patients often describe as a “mismatch” between the delicate chin and the broad posterior jaw.

Adaptation des tissus mous : pourquoi le drapage est aussi important que l’os
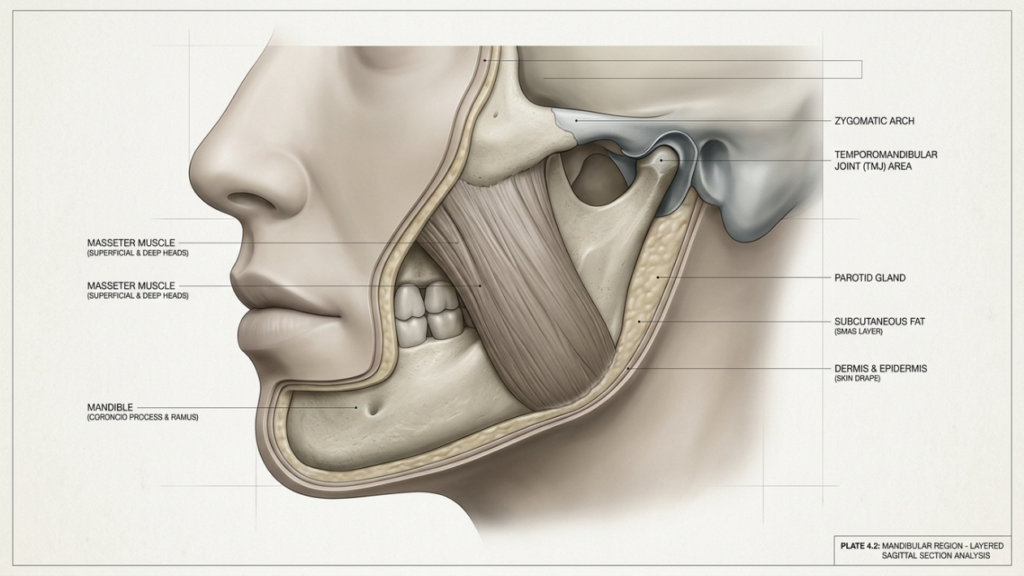
Bone is only half the equation. The soft tissue envelope—skin, subcutaneous fat, platysma, and mentalis muscle—must readapt to the new skeletal framework, and the extent of this adaptation differs dramatically between V-line jaw surgery and T-pattern genioplasty. After V-line procedures, the soft tissue envelope undergoes a prolonged redraping phase because both the mandibular angle and the chin have been altered. The masseter muscle, which inserts along the angle and ramus, must detach partially and reattach in a new position, a process that takes 8 to 12 months for full stabilization.
T-pattern genioplasty, by contrast, disturbs far less soft tissue. The mentalis muscle and chin pad are elevated and repositioned, but the masseter and parotid fascia remain untouched. Consequently, soft tissue swelling resolves faster—typically within 4 to 6 months—with more predictable early results. This difference matters for patients who need to return to professional or social environments quickly, and it also means that final aesthetic judgments should be withheld for the full redraping period appropriate to each procedure.

Le piège de la sur-résection dans la réduction de l'angle mandibulaire
Over-resection is the silent complication of réduction de l'angle mandibulaire, and it carries consequences far more visible than under-resection. Remove too much bone from the angle, and the masseter loses its attachment footprint. The muscle retracts superiorly and atrophies, creating a hollow, scooped-out appearance beneath the ear that ages the face prematurely. Worse, excessive angle removal severs the posterior buttress of the mandible, weakening the structural ring that supports the lower facial width and contributing to late-onset jowling and soft tissue ptosis.
3D morphometric data from my cohort analysis shows that patients who lost more than 10 millimeters of bigonial distance experienced a 42% increase in soft tissue sag at the jowl line within 3 years of surgery. The safe boundary for réduction de l'angle mandibulaire is typically 4 to 6 millimeters from the preoperative gonial point, preserving at least 105 degrees of gonial angle. Anything beyond this threshold ventures into over-resection territory, where the chin may look narrow and feminine, but the lateral jawline appears gaunt rather than gracefully tapered.
Stratégies de réduction du menton : ostéotomie cunéiforme ou ostéotomie en T
Both V-line jaw surgery and T-pattern genioplasty employ midline chin osteotomies to achieve chin narrowing, but the geometry of the osteotomy differs. In the V-line approach, a midline wedge osteotomy removes a triangular or trapezoidal segment of bone from the mental symphysis, allowing the lateral chin halves to slide medially. The base of the wedge sits at the inferior border, and the apex points superiorly, creating a natural taper that mirrors the feminine chin contour.
T-pattern genioplasty uses a vertical osteotomy through the horizontal genioplasty segment, splitting the chin into two halves that can be moved independently. This allows for asymmetric corrections—one half can advance while the other stays fixed—and enables precise control over chin projection. However, the vertical split creates a more abrupt medial edge that may require plate fixation and bone grafting to prevent palpable irregularities along the midline. The wedge technique, by contrast, produces a natural closing wedge approximation with broader bone-to-bone contact, which typically heals with fewer contour irregularities.
Féminisation du bas du visage : le choix de la candidate détermine le résultat
No surgical technique is superior in a vacuum; superiority is determined by patient anatomy. Lower face feminization outcomes depend on correctly matching the procedure to the skeletal phenotype. Patients with a wide bigonial distance, flared mandibular angles, and a broad chin—the classic masculine lower third—require V-line jaw surgery because addressing only the chin would leave the jaws geometrically discordant. The angle reduction restores the taper, and the chin narrowing completes the oval.
Patients whose mandibular angles are already within feminine parameters but who present with an isolated wide chin are ideal candidates for T-pattern genioplasty. Over-treating these patients with unnecessary angle reduction introduces surgical morbidity without proportional aesthetic gain and increases the risk of over-resection. Preoperative 3D photography and CT-based skeletal analysis allow precise measurement of bigonial distance, gonial angle, and mental width, enabling the surgeon to select the procedure that produces the most harmonious ratio between chin width and jawline breadth—as documented in our Avant Après FFS Galerie.

Génioplastie chez les personnes transgenres : Considérations relatives à la qualité osseuse et au drapage souple
Genioplasty transgender patients present unique anatomical considerations. Long-term hormone replacement therapy alters bone density and subcutaneous fat distribution, which affects both the surgical execution and the healing trajectory. Estrogen-dominant bone tends to be less dense than androgen-dominant bone, making osteotomies technically easier to perform but also more susceptible to over-cutting and fragmentation. The soft tissue envelope in trans women often retains thicker, more fibrous subcutaneous layers along the chin and jawline, which can mask the skeletal result for longer periods postoperatively.
In my practice, I have observed that trans women who undergo V-line jaw surgery require an average of 10.4 months for definitive soft tissue adaptation, compared to 6.2 months for cisgender women undergoing the same procedure. This extended redraping period must be communicated clearly during consultation; otherwise, patients may perceive an incomplete result at 6 months and request unnecessary revision surgery. Patience—and understanding the biomechanics of soft tissue over new bone—is essential.
Féminisation de la mâchoire : le facteur platysma
Deeper anatomy matters as much as bone. The platysma muscle spans the entire lower face, and its tone directly affects the visible result of jawline feminization. After V-line surgery, the platysma detaches from the mandibular body and must re-adhere to the new contour. If the platysma lacks adequate postoperative support—through compression garments, taping, or surgical plication—it can contract unevenly, creating banding or visible irregularities along the new jawline. T-pattern genioplasty disturbs the platysma less because the dissection remains anterior, posterior to the submandibular region.
This muscular consideration is why I frequently combine V-line jaw surgery with a limited cervicofacial approach for platysmaplasty in patients with significant laxity. The concurrent tightening secures the soft tissue envelope against the newly feminized skeleton, preventing the postoperative sag that erodes the aesthetic dividend of bone work. You can see examples of this combined approach in our documented gender transformation results.
Équation du risque nerveux : ostéotomie bilatérale ou antérieure
The inferior alveolar nerve (IAN) follows a course through the mandibular ramus and body, exiting at the mental foramen below the second premolar. V-line jaw surgery places osteotomies in two zones adjacent to the IAN: the mandibular angle cut, which runs posterior to the foramen, and the chin narrowing cut, which passes through the symphysis anterior to the foramen. T-pattern genioplasty places osteotomies only in the anterior zone. Consequently, the nerve injury profile differs: V-line surgery carries a reported temporary paresthesia rate of 28–35% (bilateral), while T-pattern genioplasty carries a temporary rate of 12–18% (bilateral).
Permanent nerve injury remains rare in both procedures when performed by experienced surgeons—below 2% in published series—but the broader exposure of the V-line approach means the surgeon must protect the nerve at two separate anatomical locations rather than one. This dual-vulnerability is one reason why meticulous subperiosteal dissection and intraoperative nerve monitoring are standard protocols in mandibular contouring at our facility.
Guide de décision étape par étape pour votre intervention chirurgicale
Choisir entre V-line jaw surgery and T-pattern genioplasty requires a structured, data-driven evaluation. Follow this decision framework to determine which lower-face feminization strategy is correct for your anatomy:
1. Mesurez votre distance bigoniale à l'aide de l'imagerie 3D
Obtain a 3D CT scan of your facial skeleton. Measure the distance between the two gonial points. A bigonial distance exceeding 95 millimeters in a facial framework consistent with male skeletal proportions typically indicates the need for mandibular angle reduction as part of the surgical plan. Values below 90 millimeters suggest the angles are already within a feminine range and T-pattern genioplasty alone may suffice.
2. Évaluez votre angle gonial
Measure the gonial angle on the lateral cephalometric view. Masculine mandibles typically range from 115 to 130 degrees. Feminine mandibles average 125 to 140 degrees. If your gonial angle is below 120 degrees, angle reduction through V-line jaw surgery will likely produce a more natural transition than chin narrowing alone.
3. Évaluer la largeur du menton par rapport à la conicité de la mâchoire
Compare the transverse width of the mental symphysis to the bigonial distance. If the chin appears broad disproportionately to already-feminine angles, T-pattern genioplasty directly targets the issue. If both the chin and angles are wide, V-line jaw surgery addresses the entire contour simultaneously.
4. Calculer le temps de récupération acceptable des tissus mous
Determine your professional and social timeline. V-line jaw surgery requires 8 to 12 months for full soft tissue adaptation, while T-pattern genioplasty stabilizes in 4 to 6 months. Plan your surgery around your life commitments accordingly.
5. Analyser les résultats obtenus chez de vrais patients
Examine before-and-after photographs from your surgeon, specifically looking at the chin-to-jaw transition zone. Pay attention to whether the jawline flows smoothly from angle to chin or whether a visible step-off exists. You can review dozens of real patient outcomes in our comprehensive body feminization results gallery.
6. Discuter des risques nerveux et des limites de la résection excessive
During your consultation, explicitly ask your surgeon how much bone they plan to remove at the angle and chin, what their over-resection rate is, and how they protect the inferior alveolar nerve during osteotomy. A qualified surgeon will provide specific millimeter targets and explain their safety margins.
7. Soumettez votre demande d'évaluation personnalisée
Every face is unique, and no algorithm replaces individualized surgical planning. Take the first step toward your transformation by completing our evaluation form so we can analyze your anatomy and recommend the procedure that maximizes your aesthetic outcome while minimizing risk.
Your lower face tells a story of identity, confidence, and transformation—ensure that story is written by an experienced hand. Apply now for your personalized surgical assessment and take the definitive step toward the feminine jawline you envision.
Questions fréquemment posées
Quelle est la principale différence entre une chirurgie de la mâchoire en V et une génioplastie en T ?
La chirurgie maxillaire en V associe la réduction de l'angle mandibulaire à un affinement du menton et à une génioplastie en une seule intervention, tandis que la génioplastie en T affine uniquement le menton sans modifier les angles mandibulaires. La technique en V traite l'ensemble du tiers inférieur du visage ; la technique en T cible uniquement le menton.
Quelle procédure permet d'obtenir une transition menton-mâchoire plus naturelle ?
La chirurgie de la mâchoire en V permet une transition menton-mâchoire plus harmonieuse et continue, car elle sculpte simultanément l'angle mandibulaire et le menton. La génioplastie en T peut, quant à elle, laisser un aspect asymétrique visible si les angles restent larges alors que le menton est affiné indépendamment.
Dans quelle mesure chaque procédure permet-elle de réduire la largeur du menton ?
La chirurgie de la mâchoire en V permet une réduction moyenne de la largeur du menton d'environ 7,2 millimètres, tandis que la génioplastie en T permet une réduction d'environ 5,8 millimètres. L'approche en V permet un rétrécissement plus important car les angles sont réduits proportionnellement.
Pourquoi la sur-résection est-elle un problème lors de la réduction de l'angle mandibulaire ?
Une résection excessive de l'angle mandibulaire entraîne la suppression de l'insertion du muscle masséter, provoquant un creusement et un vieillissement prématuré du visage. Cette résection excessive fragilise également l'anneau structurel mandibulaire, ce qui induit un relâchement des tissus mous, un affaissement des bajoues et un aspect émacié et artificiel.
Combien de temps dure la récupération des tissus mous après chaque intervention ?
La chirurgie de la mâchoire en V nécessite 8 à 12 mois pour une adaptation complète des tissus mous, car l'angle et le menton sont modifiés. La génioplastie en T se stabilise généralement en 4 à 6 mois, car le masséter et les tissus mous latéraux restent intacts.
Qui est le candidat idéal pour une génioplastie en T isolée ?
Les patientes présentant des angles mandibulaires naturellement féminins, mais un menton large ou carré isolé, sont des candidates idéales. Leur contour mandibulaire étant déjà effilé, un affinement du menton sans réduction des angles permet d'éviter une morbidité chirurgicale inutile et un risque de résection excessive.
En quoi le risque d'atteinte nerveuse diffère-t-il entre ces deux interventions ?
La chirurgie maxillaire en V consiste à pratiquer des ostéotomies à proximité du nerf alvéolaire inférieur à deux endroits : postérieurement au niveau de l’angle et antérieurement au niveau du menton, ce qui entraîne une paresthésie temporaire dans 28 à 35 % des cas (TP3T). La génioplastie en T n’aborde le nerf que par voie antérieure, avec un taux de paresthésie temporaire de 12 à 18 % (TP3T).
L'hormonothérapie peut-elle influencer le résultat chirurgical de ces interventions ?
Oui. Un traitement hormonal substitutif à long terme modifie la densité osseuse et la répartition du tissu adipeux sous-cutané, ce qui facilite les ostéotomies mais augmente le risque de fragmentation. Les femmes transgenres nécessitent généralement une période d'adaptation des tissus mous plus longue (environ 10 mois) que les femmes cisgenres subissant la même intervention.