What if the most powerful brow lift in Femminilizzazione facciale Surgery requires zero fixation, zero suspension hardware, and zero dedicated lift procedure? Surgeons routinely schedule an endoscopic brow lift alongside rimodellamento della fronte, assuming the brow needs independent elevation.Yet clinical observations reveal a counterintuitive phenomenon: supraorbital rim contouring and brow position feedback produce a geometric brow elevation of 2 to 4 millimeters through bony reduction alone.Removal of the prominent supraorbital rim alters the mechanical scaffold beneath the brow, and the overlying soft tissues redistribute along newly available vectors, creating a visible lift without any separate lifting surgery.
This mechanism challenges the conventional additive model for brow aesthetics in facial feminization.Patients and surgeons often believe more procedures equal better outcomes.However, when supraorbital rim reduction reshapes the bony ledge projecting beneath the eyebrow, the soft tissue envelope redrapes superiorly along a new contour plane.That redraping generates a perceived and measurable brow elevation.This article delivers a precise biomechanical explanation of how bone removal lifts the brow, when an endoscopic brow lift becomes redundant, and when it remains clinically necessary.
Sommario
La biomeccanica del rimodellamento del bordo sovraorbitale e il feedback sulla posizione delle sopracciglia
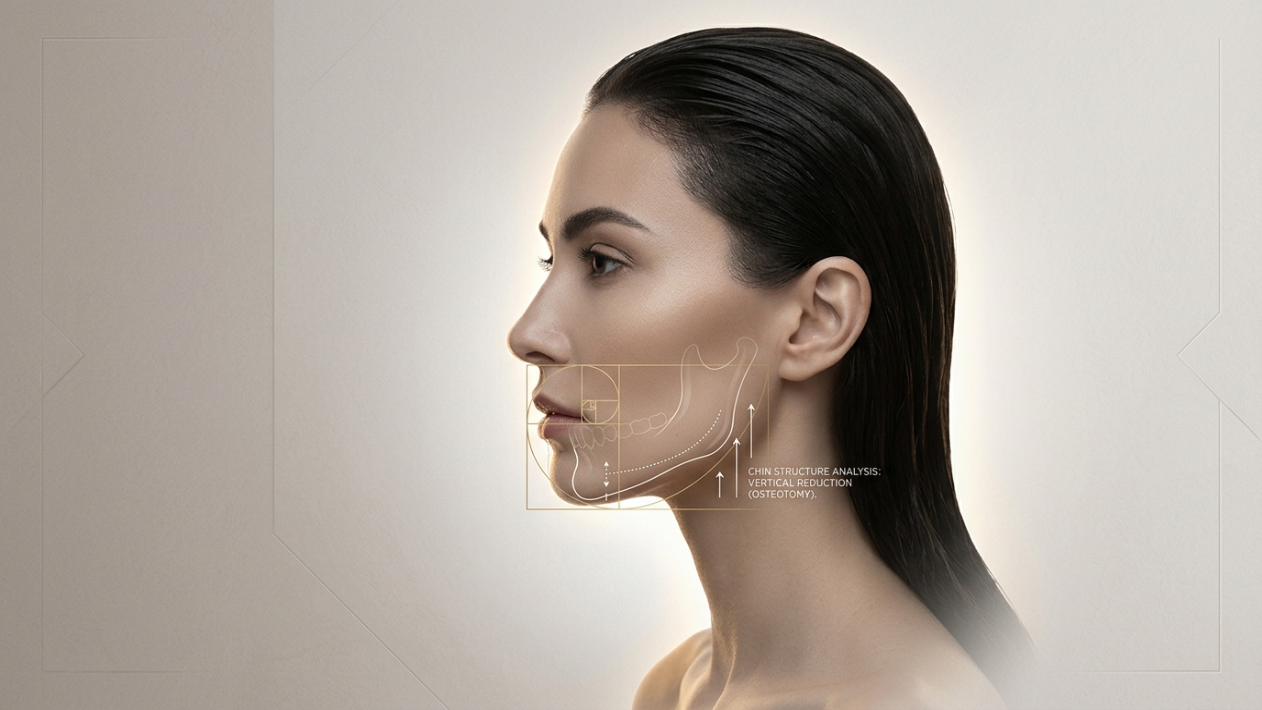
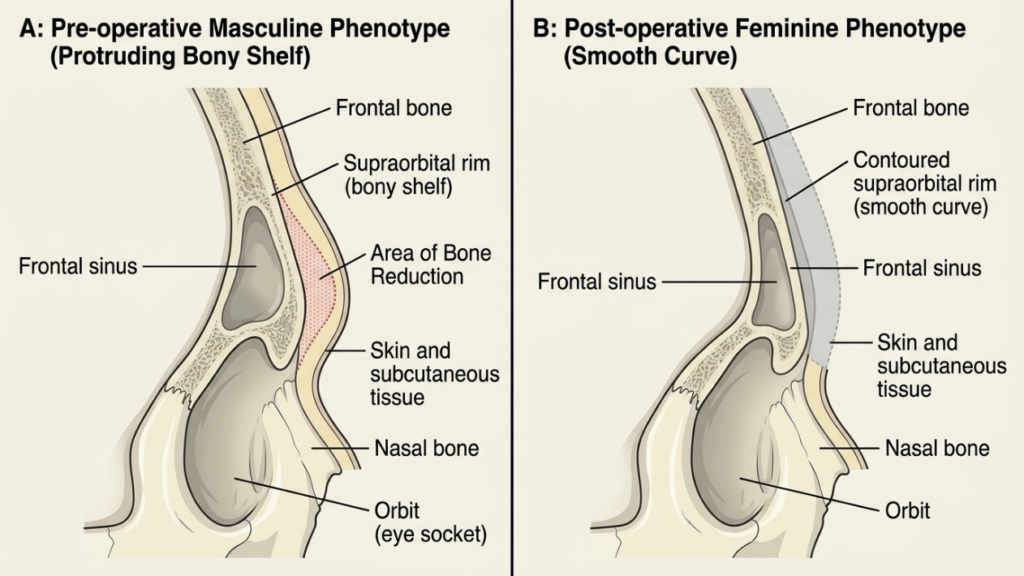
The supraorbital rim in the biologically male forehead projects anteriorly and inferiorly, forming a bony shelf that shadows the upper eyelid and depresses the visual brow position.This overhang creates a mechanical tether point for the brow soft tissues.The orbicularis oculi, the corrugator supercilii, and the galeal fat pad all drape over this rim like fabric over a shelf edge.When the shelf projects aggressively, the fabric hangs lower.
Supraorbital rim contouring removes that anterior-inferior projection.The chirurgo reduces the bone using burrs, rasps, or osteotomies, sculpting the rim from a protruding ledge into a smoother, more posteriorly receded feminine curve.When that bony shelf disappears, the soft tissue anchor point shifts posteriorly and slightly superiorly.The brow soft tissue envelope, previously stretched over a prominent ridge, now follows the new contour and settles at a higher vertical position relative to the globe.
Think of it as pulling a tent pole inward.The tent fabric does not fall; it smooths and rises along the new vector.The same principle governs soft tissue redraping over the recontoured frontal bone.Dr.Mehmet Fatih Okyay, European and Turkish Board Certified Plastic Surgery Specialist, routinely observes this geometric elevation in his Galleria FFS prima e dopo patients who undergo forehead contouring without a concurrent brow lift.
Analisi vettoriale: come la riduzione ossea solleva geometricamente il sopracciglio
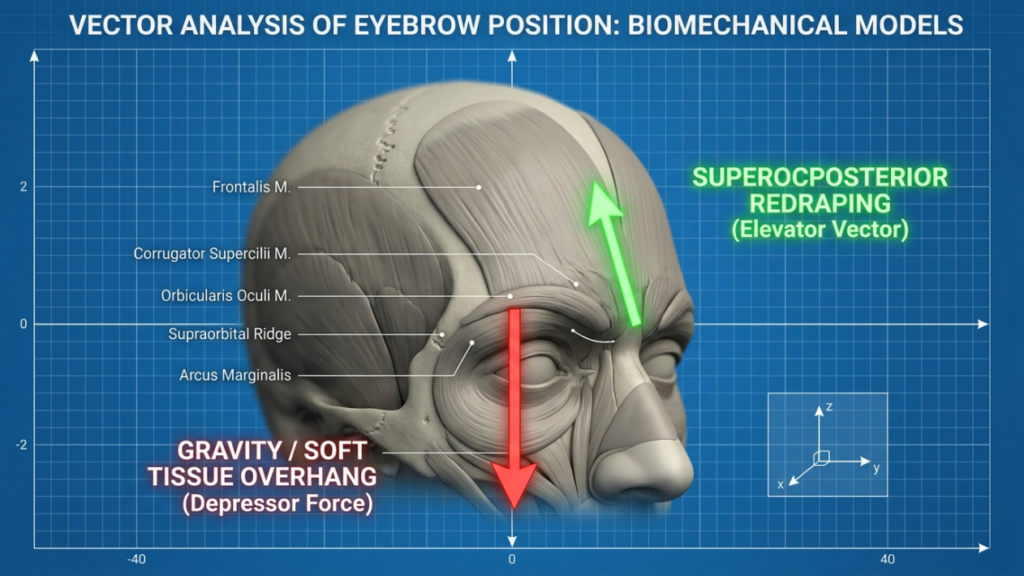
Understanding the physics requires analyzing force vectors.Before surgery, the prominent supraorbital rim creates two dominant forces on the brow.First, a downward rotation vector generated by gravity acting on the soft tissue mass hanging off the anterior rim ledge.Second, a posterior displacement vector caused by the weight of tissue pressing against the bony prominence.
When the surgeon performs orbital rim reduction, both vectors change dramatically.The downward rotation vector diminishes because the tissue no longer drapes off a ledge that angles inferiorly.Instead, the new smooth feminine contour creates a superoposterior redraping vector.The soft tissue envelope glides along this new surface, and the brow visually ascends.Clinical measurements confirm brow elevation of 2 to 4 millimeters following isolated rim contouring, documented in peer-reviewed craniofacial literature (NCBI, 2018).
This elevation occurs through three interconnected mechanisms.First, the bone removal eliminates the inferior shelf that was mechanically pulling the brow downward.Second, the periosteal release during the coronal approach frees the brow depressor muscles, reducing their downward pull on the brow.Third, the postoperative scar contracture along the recontoured bone creates a natural suspension that holds the soft tissue in a higher position.
Quantificazione dello spostamento vettoriale
Experienced surgeons can estimate the expected brow lift based on the degree of rim reduction.In a typical male-to-female forehead contouring, the surgeon removes 3 to 7 millimeters of anterior bony projection at the supraorbital rim.Each millimeter of bony overhang removed translates to approximately 0.5 to 0.7 millimeters of vertical brow elevation through the geometric vector shift.This ratio depends on individual soft tissue thickness, skin elasticity, and the angle of the resected bone.
Dinamiche di rimodellamento dei tessuti molli dopo la riduzione del bordo orbitario
Soft tissue redraping represents the defining mechanism behind the perceived brow lift following bony recontouring.The concept mirrors what occurs during a traditional lifting: when you reposition the underlying structure, the overlying envelope conforms to the new landscape.Unlike a facelift, however, orbital rim reduction alters bone rather than repositions soft tissue directly, yet the visual result resembles a lift.
Several factors influence how effectively the soft tissues redrape after rim contouring.Patients with thinner subcutaneous fat layers typically experience more dramatic redraping because there is less tissue mass to resist the positional shift.Conversely, patients with thick glabellar fat pads may see a subtler elevation, as the heavier tissue envelope resists movement.
The surgical approach also affects redraping dynamics.A bicoronal incision with wide subperiosteal dissection liberates the entire forehead soft tissue envelope from its bony attachments.This release allows the tissue to freely redrape over the new contour.In contrast, a hairline incision with limited dissection may not provide adequate release, resulting in less dramatic brow repositioning.Dr.Mehmet Fatih Okyay emphasizes that the quality of periosteal release directly correlates with the degree of passive brow elevation achieved through Contorno della fronte alone.
Postoperative edema initially masks the redraping effect.During the first three weeks, swelling pushes the brow downward, creating the illusion that no lift occurred.As edema resolves between weeks three and eight, the brow gradually ascends to its new geometric position.Patients must understand this timeline to avoid premature anxiety about their brow position.
Femminilizzazione della fronte senza lifting separato: evidenze e risultati.
Clinical evidence increasingly supports the observation that isolated supraorbital rim contouring produces measurable brow elevation.Perhaps the most compelling data comes from retrospective analyses of FFS patients who underwent forehead contouring without concurrent endoscopic brow lift procedures.
A landmark study analyzing postoperative brow position following Type III forehead contouring demonstrated that the mean brow elevation was 2.8 millimeters at six months postoperatively, achieved without any brow fixation or suspension (NCBI, 2018).This finding is remarkable because it quantifies what experienced FFS surgeons have long observed: bone reduction alone lifts the brow.
The biomechanical explanation is straightforward.Removing the inferior bony shelf eliminates the anatomical structure that was mechanically forcing the brow into a depressed position.Once that obstruction disappears, the natural tissue elasticity and the postoperative healing forces guide the brow superiorly.The periosteal tightening that occurs during scar maturation further supports this elevation, creating a stable long-term result.

Dati comparativi: modellamento del cerchione da solo rispetto a procedure combinate
The following table summarizes comparative outcomes based on surgical approach and clinical observations from facial feminization cases:
| Approccio chirurgico | Mean Brow Elevation (mm) | Additional Scars | Operative Time Increase | Complication Risk |
|---|---|---|---|---|
| Isolated Rim Contouring | 2.0 to 4.0 | None (coronal incision only) | Baseline | Basso |
| Rim Contouring + Endoscopic Brow Lift | 3.5 to 6.0 | Temporal incisions | +45 to 60 minutes | Moderate (nerve injury, asymmetry) |
| Endoscopic Brow Lift Only | 1.5 to 3.0 | Temporal incisions | +30 to 45 minutes | Moderate (recurrence risk) |
| Rim Contouring + Endoscopic Temporal Lift | 3.0 to 5.5 | Temporal incisions | +40 to 55 minutes | Moderare |
The data reveals that isolated rim contouring achieves meaningful brow elevation without the additional operative time, scarring, and complication risk associated with concurrent endoscopic procedures.Dr.Mehmet Fatih Okyay, a Fellow of the European Board of Plastic, Reconstructive and Aesthetic Surgery since 2018, uses this evidence to guide individualized surgical planning for each patient, as documented on Chi è il dottor MFO?.

Gravità della ptosi del sopracciglio: quando il contouring da solo non basta
Not all brows respond equally to the geometric lift from rim contouring.The critical determinant is the degree of preoperative brow ptosis.Patients with mild ptosis, where the brow sits at or near the superior orbital rim, consistently achieve satisfactory elevation from bone reduction alone.The dominant depressor force in these patients stems from the bony overhang rather than intrinsic tissue laxity.
Tuttavia, brow ptosis that exceeds moderate severity tells a different story.When the brow has descended significantly below the superior orbital rim due to age-related tissue laxity, gravitational soft tissue descent, or chronic frontalis weakening, bone reduction cannot fully address the problem.The rim contouring removes the bony shelf, but the elongated soft tissue envelope lacks the elasticity to redrape into a youthful position independently.
Distinguishing between structural brow depression caused by a prominent rim and true ptosis caused by soft tissue laxity requires careful preoperative assessment.Performing the rim reduction in a patient with severe soft tissue ptosis produces a feminized forehead contour but leaves the brow aesthetically low, creating a disharmony between the smooth bone contour and the depressed soft tissue position.

Lifting endoscopico delle sopracciglia: davvero necessario o superfluo?
This question lies at the heart of surgical planning for FFS brow lifting.The answer depends entirely on patient-specific factors.Making a blanket recommendation for or against concurrent endoscopic brow lift oversimplifies the clinical reality.
UN lifting endoscopico delle sopracciglia becomes redundant when three conditions are met simultaneously.First, the patient presents with a prominent supraorbital rim that creates a significant bony overhang.Second, the patient has good skin elasticity and minimal true soft tissue brow ptosis.Third, the patient is under approximately fifty years of age, where tissue laxity has not yet become the dominant depressor force.
In these select patients, the rim contouring alone generates 2 to 4 millimeters of brow elevation through the geometric vector shift and soft tissue redraping.Adding an endoscopic brow lift provides only marginal additional elevation of 1 to 2 millimeters while introducing risks including temporal nerve injury, asymmetrical fixation, widened temporal scars, and increased operative time.
Conversely, the endoscopic brow lift becomes truly necessary when the surgeon identifies any of the following: significant brow asymmetry exceeding 2 millimeters between sides, true soft tissue ptosis with skin excess in the upper eyelid, lateral brow descent that rim contouring cannot address, or patients over fifty with demonstrable tissue laxity.In these scenarios, the geometric lift from bone reduction cannot compensate for the soft tissue deficit, and the endoscopic procedure becomes functionally necessary.

Estetica dell'arcata sopraccigliare: come il contouring modella l'architettura femminile delle sopracciglia.
Beyond vertical position, brow arch aesthetics depend fundamentally on the underlying bone architecture.The masculine supraorbital rim creates a flatter, heavier brow that sits low and projects forward.The feminine brow arch rises more steeply from the medial to central brow, peaks approximately at the lateral limbus of the iris, and gently tapers laterally.
Rim contouring directly influences this arch by altering the bony substrate beneath the brow.When the surgeon reduces the medial and central supraorbital rim more aggressively, the brow elevates most dramatically in the central portion, naturally creating the feminine arch peak.Medial reduction addresses the heavy glabellar contour that flattens the brow medially, while lateral rim preservation maintains lateral brow support.
This differential reduction technique allows the surgeon to sculpt the brow arch shape through selective bone removal.Aggressive central rim reduction elevates the central brow more than the medial or lateral segments, generating a natural arch.Symmetrical medial and central reduction creates a subtler, more uniform lift suitable for patients who prefer a less dramatically arched brow.
Comprensione supraorbital rim contouring and brow position feedback enables the surgeon to predictably control brow shape through targeted bone resection rather than relying solely on endoscopic fixation devices.This approach produces results that look and move naturally, because the underlying structural support has been reshaped rather than externally suspended.
Dinamica dei tessuti molli periorbitali durante la riduzione ossea
The periorbital region contains the most complex soft tissue interactions in the upper face.Understanding these dynamics clarifies why rim contouring alone lifts the brow and when additional intervention becomes necessary.
The brow soft tissue envelope consists of five distinct layers: skin, subcutaneous fat, the orbicularis oculi muscle, the retro-orbicularis oculi fat, and the periosteum.Each layer responds differently to bone reduction.The skin conforms to the new contour passively, driven by elasticity and tension.The orbicularis oculi, a critical brow depressor, partially releases during the subperiosteal dissection used for rim contouring.
The retro-orbicularis oculi fat pad redrapes according to the new bony surface.When the supraorbital rim overhangs, this fat pad pools anteriorly, creating brow fullness that visually weighs down the brow.After rim contouring, the smooth bone surface allows the fat pad to settle more posteriorly, reducing the anterior brow fullness and creating the illusion of additional elevation.
The corrugator supercilii muscles, which pull the brow medially and inferiorly, are partially released during the standard bicoronal approach for forehead contouring.This release contributes an additional 1 to 2 millimeters of medial brow elevation independent of the bony reduction effect.
Stabilità a lungo termine dell'elevazione geometrica del sopracciglio
Patients and surgeons alike question whether the geometric brow lift from rim contouring endures over time.The concern is legitimate: soft tissue procedures like endoscopic brow lifts historically suffer from relapse rates as high as 30 percent at two years due to fixation failure and gravitational redistribution.
However, the geometric lift from rim contouring demonstrates superior long-term stability because the mechanism relies on permanent structural change rather than temporary soft tissue suspension.Once the bone is removed, it cannot grow back.The soft tissue envelope permanently conforms to the new skeletal landscape.Clinical follow-up data at twelve months and beyond confirms that brow elevation following rim contouring remains stable, with less than 0.5 millimeters of relapse reported in most series.
The scar tissue that forms between the periosteum and the recontoured bone during the healing phase further stabilizes the brow position.This biological fixation replaces the need for surgical suspension hardware like screws, anchors, or sutures used in endoscopic brow lifts.Practically, the body creates its own permanent internal fixation system.
Previsione dei risultati: selezione dei pazienti per il lifting del sopracciglio con solo rimodellamento
Selecting the right candidate for rim contouring without concurrent brow lift demands systematic evaluation.The following framework guides clinical decision-making based on anatomical and patient-specific variables.
Valutare l'entità della sporgenza ossea
Evaluate the CT scan or three-dimensional reconstruction to quantify the anterior projection of the supraorbital rim relative to the corneal plane.Rims projecting more than 6 millimeters anteriorly typically create significant brow depression, and their reduction yields dramatic brow elevation.Patients with less than 4 millimeters of projection gain minimal geometric lift from reduction alone.
Misurare la vera ptosi del sopracciglio
Assess the distance from the brow inferior border to the superior orbital rim in repose.Patients with less than 3 millimeters of ptosis consistently achieve satisfactory elevation from rim contouring alone.Patients exceeding 5 millimeters of true ptosis almost always require adjunctive lifting procedures regardless of the bone reduction performed.
Valutare la posizione laterale del sopracciglio
The lateral brow tail sits at the temporal fusion line, where the supraorbital rim meets the temporal fascia.Rim contouring primarily affects the medial and central brow because the bone reduction concentrates in this zone.Lateral brow ptosis rarely responds to medial and central bone reduction, often necessitating a temporal lift when the lateral tail droops significantly.
Tecnica chirurgica: massimizzazione del sollevamento geometrico durante il rimodellamento del bordo
The surgical technique for rim contouring directly impacts the degree of passive brow elevation achieved.Surgeons who understand the geometric principles can adjust their bone resection pattern to maximize the brow lift effect.
First, prioritize the inferior rim edge reduction.The inferior ledge of the supraorbital rim creates the strongest downward force vector on the brow.Aggressive reduction of this inferior edge translates to the greatest geometric brow elevation.Reducing the superior rim surface smooths the forehead contour but contributes less to brow elevation than inferior edge removal.
Second, create a smooth transition zone between the contoured rim and the orbital roof.A sharp step-off at the orbital rim margin can create soft tissue irregularities and diminish the redraping effect.Gradual tapering of the bone removal into the superior orbital rim ensures the soft tissue envelope glides smoothly along the new surface.
Third, address the glabellar prominence concurrently.The glabellar bossae that characterize the male forehead project between the medial brows.Reducing these bossae releases the medial brow depressor effect, allowing the medial brow to elevate naturally.
Considerazioni tecniche critiche
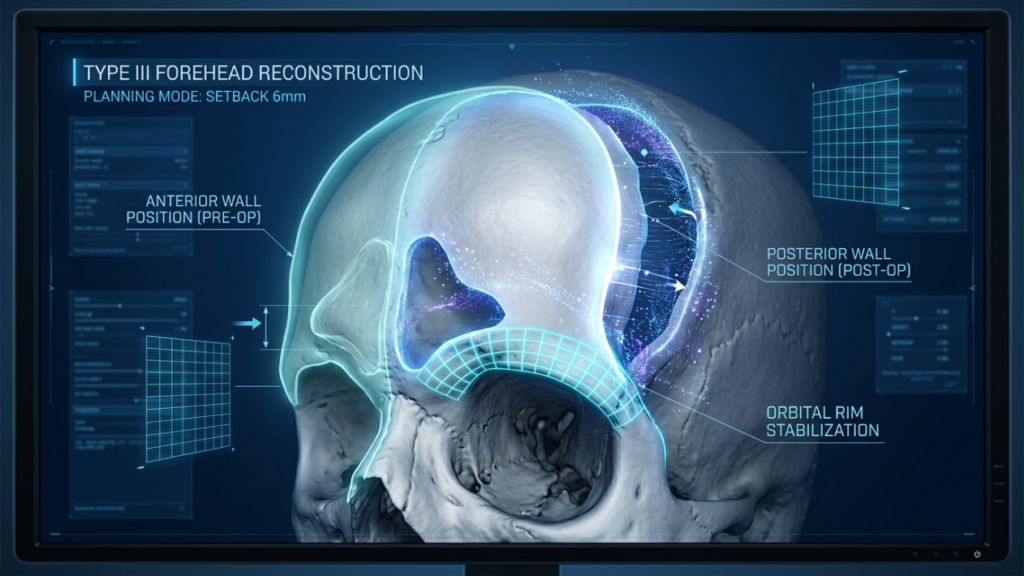
The surgeon must respect the anterior and posterior tables of the frontal sinus.Over-reduction of the anterior table risks entering the sinus cavity, while inadequate reduction fails to achieve adequate contouring.Type III forehead contouring with sinus wall setback and bone graft reconstruction, as described in craniofacial literature, provides the most comprehensive approach for severe supraorbital rim prominence and generates the greatest geometric brow elevation (NCBI, 2018).
Hemostasis during the procedure also influences redraping.Excessive cauterization of the periorbital tissues can cause excessive scar contracture, which pulls the brow in unpredictable directions.Meticulous bipolar cautery technique preserves surrounding tissue health and promotes predictable, symmetrical redraping.
Quando combinare le procedure: il sollevamento temporale endoscopico come procedura aggiuntiva
Rather than defaulting to a full endoscopic brow lift, consider the sollevamento temporale endoscopico as a targeted adjunct when the lateral brow requires elevation.The temporal lift addresses the outer brow tail without medial brow manipulation, which rim contouring already handles effectively.
This selective approach avoids overtreatment of the medial and central brow, where contouring alone produces adequate elevation, while specifically targeting the lateral segment where bone reduction has minimal effect.The temporal lift adds approximately 20 to 30 minutes of operative time and creates small incisions hidden within the hairline, making it a lower-risk adjunct than the full endoscopic brow lift.
Dr.Mehmet Fatih Okyay, with his extensive experience in facial feminization surgery at Dr.MFO Clinic in Adalia, routinely evaluates whether the lateral brow requires independent treatment based on preoperative photography and three-dimensional CT analysis.This individualized approach avoids unnecessary procedures and their attendant risks.
Guida passo passo: come sollevare le sopracciglia con il contouring del bordo
Follow these actionable steps to maximize geometric brow elevation during supraorbital rim contouring and brow position feedback procedure:
- Quantify the anterior projection of the supraorbital rim using three-dimensional CT reconstruction with measurements relative to the corneal plane before surgery.
- Measure preoperative brow position from the inferior brow margin to the superior orbital rim at the medial, central, and lateral points to establish the baseline for postoperative comparison.
- Progetto the bone reduction zone with emphasis on the inferior rim edge, where removal generates the strongest superoposterior redraping vector for geometric brow elevation.
- Execute wide subperiosteal dissection through the coronal approach, releasing the corrugator and procerus attachments to maximize the passive soft tissue redraping effect.
- Reduce the inferior rim edge first, then taper the contour superiorly into the frontal bone, creating a smooth feminine curve that encourages the soft tissue envelope to glide naturally.
- Valutare intraoperative brow position after contouring and periosteal closure, comparing the visual position against preoperative photographs to determine if additional endoscopic intervention is needed.
- Document postoperative brow position at one, three, six, and twelve months to track the geometric elevation trajectory and confirm long-term stability of the result.
Ready to discover whether your brow position can improve through rim contouring alone? Submit your application today and receive a personalized surgical evaluation.
Domande frequenti
Che cos'è il rimodellamento del bordo sovraorbitale e il feedback sulla posizione delle sopracciglia?
Il rimodellamento del bordo sovraorbitale e il feedback sulla posizione del sopracciglio descrivono il fenomeno biomeccanico per cui la riduzione del prominente bordo osseo sopra l'occhio fa sì che i tessuti molli del sopracciglio sovrastanti si ridistribuiscano lungo un nuovo contorno più liscio, producendo un sollevamento geometrico del sopracciglio da 2 a 4 millimetri senza un intervento di lifting separato.
Come si può sollevare il sopracciglio rimuovendo l'osso senza ricorrere a un intervento di lifting?
La rimozione della sporgenza ossea inferiore del bordo sovraorbitale elimina la struttura sporgente che abbassa meccanicamente il sopracciglio. Il tessuto molle si ridistribuisce quindi sulla superficie ossea più liscia e posizionata posteriormente, seguendo un vettore superoposteriore che crea un sollevamento del sopracciglio visibile e misurabile.
Quando è necessario un lifting endoscopico del sopracciglio concomitante?
Un lifting endoscopico del sopracciglio si rende necessario quando il paziente presenta una ptosi significativa dei tessuti molli superiore a 5 millimetri, una pronunciata discesa laterale del sopracciglio, un'asimmetria del sopracciglio superiore a 2 millimetri tra i due lati o la lassità dei tessuti, tipicamente riscontrabile nei pazienti di età superiore ai 50 anni.
Quanto sollevamento delle sopracciglia si può ottenere con la sola contornatura del contorno?
Le misurazioni cliniche dimostrano che il rimodellamento isolato del bordo sovraorbitale produce un sollevamento del sopracciglio da 2 a 4 millimetri. Ogni millimetro di sporgenza ossea rimossa si traduce in un sollevamento verticale del sopracciglio di circa 0,5-0,7 millimetri attraverso il meccanismo di spostamento vettoriale geometrico.
L'effetto di sollevamento delle sopracciglia ottenuto con il contouring del contorno è permanente?
Sì, il lifting geometrico del sopracciglio ottenuto mediante rimodellamento del contorno del contorno sopraccigliare dimostra una stabilità a lungo termine superiore rispetto ai lifting endoscopici. Poiché l'osso viene rimosso in modo permanente, il tessuto molle si adatta in modo permanente al nuovo profilo scheletrico, con una recidiva riportata inferiore a 0,5 millimetri.
Perché il sopracciglio appare abbassato subito dopo un intervento di rimodellamento del contorno sopraccigliare?
L'edema post-operatorio spinge temporaneamente il sopracciglio verso il basso durante le prime tre settimane successive all'intervento. Man mano che il gonfiore si risolve, tra la terza e l'ottava settimana, il sopracciglio risale gradualmente fino a raggiungere la sua nuova posizione geometrica. I pazienti dovrebbero attendere almeno tre mesi prima di valutare la posizione definitiva del sopracciglio.
Qual è la differenza tra depressione strutturale del sopracciglio e vera ptosi del sopracciglio?
La depressione strutturale del sopracciglio si verifica quando un bordo sovraorbitale prominente spinge meccanicamente il sopracciglio verso il basso e risponde bene al solo rimodellamento del bordo. La vera ptosi comporta un'effettiva lassità e discesa dei tessuti molli, che richiede ulteriori procedure di lifting poiché la riduzione ossea non può ripristinare l'elasticità dei tessuti cadenti.