Why does a 5,000-graft FUE procedure still leave a 43-year-old trans woman looking unmistakably masculine in the forehead? The answer devastates most patients when they first hear it: haartransplantatie alone cannot recreate a feminine hairline in a skull reshaped by decades of testosterone. Even the most meticulous follicular unit extraction fails when it must fill a frontotemporal recession spanning five centimeters on each temple. The grafts survive, the hair grows, yet the face remains framed by a stubbornly male pattern.
Correcting receding hairline in trans women over 40 demands a fundamentally different approach than simply transplanting follicles into bald skin. The bald temporal triangles represent not just lost hair but repositioned tissue—the scalp has literally migrated posteriorly under androgenic influence. Without physically pulling that scalp forward first, FUE grafts populate an anatomically male frame with hair that can never achieve the rounded, low-set feminine contour. This article presents the combined surgical scalp advancement plus FUE protocol developed through years of clinical refinement at Dr. MFO Clinic, demonstrating why staged intervention creates results that isolated transplantation cannot.
Inhoudsopgave
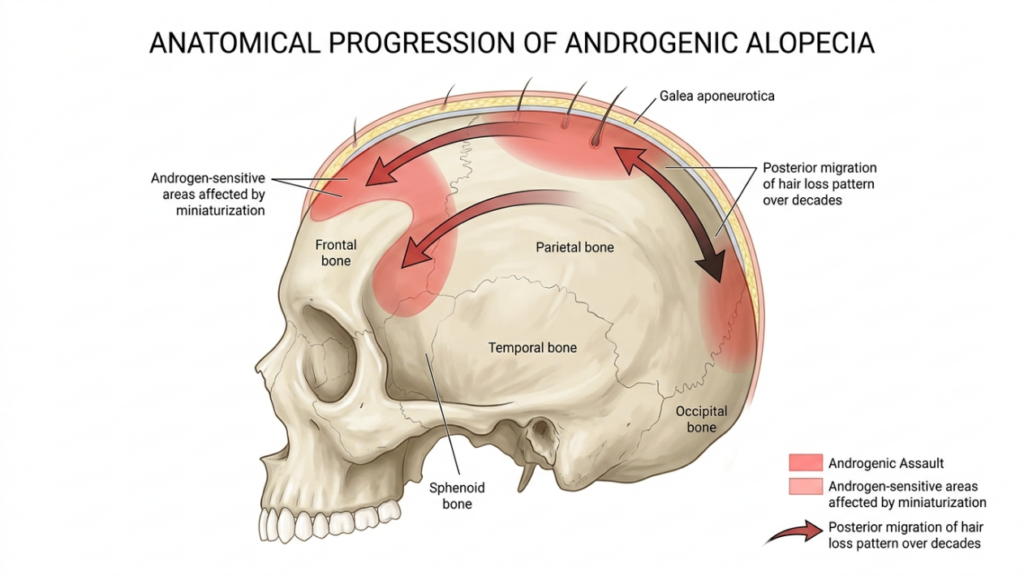
De androgene aanval: inzicht in frontotemporale recessie bij de ouder wordende transvrouw
Before age 30, the hairline sits at a predictable position, and even male-pattern recession remains relatively contained. After 40, however, frontotemporal recession accelerates dramatically, driven by cumulative dihydrotestosterone exposure that progressively miniaturizes follicles along the temporal peaks and anterior scalp. For trans women who initiated hormone therapy later in life, the damage extends far beyond what estrogen reversal can accomplish. According to a landmark study published in the International Journal of Transgenderism, hormone replacement therapy halts further loss but regrows hair in fewer than 30 percent of patients with Norwood grade III recession or higher, and virtually zero patients see significant regrowth in the temporal horns (International Journal of Transgenderism, 2014).
This data point carries enormous consequences. A trans woman over 40 presenting with Norwood III–IV frontotemporal recession typically lacks sufficient donor density to cover both temporal voids while maintaining donor-site integrity. Each temporal triangle requires approximately 1,500–2,000 grafts to create convincing density. Multiply that demand across both temples, add the central forelock requirement, and the graft count exceeds 4,500—a number that pushes most donor zones past safe extraction limits.
Waarom FUE alleen een onnatuurlijke dichtheidsverdeling oplevert
Performing isolated FUE on advanced frontotemporal recession creates three distinct aesthetic failures that surgeons rarely discuss in consultation rooms. First, the density distribution appears wrong. A feminine hairline transitions gradually from dense central forelock hair at the midpoint, through decreasing density along the temples, into fine vellus-like single-hair grafts at the hairline edge. When transplanting into entirely bald temporal triangles, surgeons must pack grafts densely across a wide area, resulting in uniform density that looks artificial against the natural progressive-thinning gradient of surrounding native hair.

Second, the hairline position remains too high. Even with 2,000 temporal grafts, the lowest possible hairline position equals the bald skin boundary minus one millimeter—the graft must sit in existing skin. In a patient whose hairline has receded four centimeters, FUE can only place hair starting at that four-centimeter mark, which still leaves a high, masculine forehead. No amount of transplanted density lowers that anatomical border.
Third, the temporal recession angles pose a graft-direction nightmare. Temporal hair grows at extremely flat angles against the skin, sometimes nearly parallel to the scalp surface. FUE recipient sites in bald temporal skin frequently create grafts that emerge at steeper angles than native temporal hair, producing an incongruent visual where transplanted tufts visibly differ from surrounding growth patterns.
De Norwood-classificatie en de transvrouw boven de 40: een aangepaste beoordeling
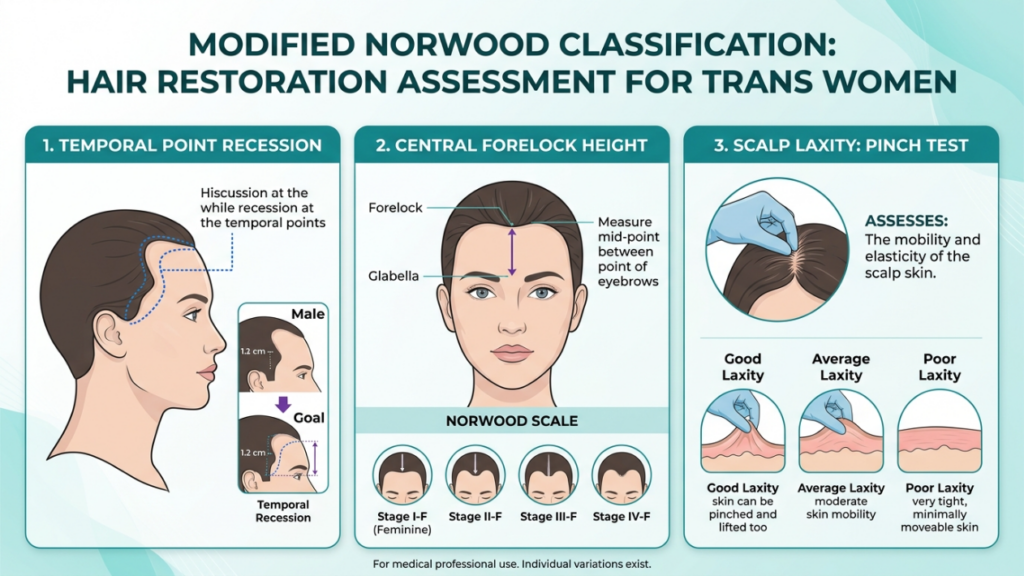
The classic Norwood classification system describes male pattern baldness along a I–VII spectrum. For trans women over 40, Dr. MFO applies a modified assessment that specifically evaluates three parameters the standard Norwood scale ignores: temporal point recession depth, central forelock height relative to the glabella, and scalp laxity in the frontal band. These three factors determine whether FUE alone can succeed or whether combined surgical hairline restoration becomes necessary.
Patients at modified Norwood I–II typically have less than two centimeters of recession and adequate scalp laxity. These patients can achieve satisfactory feminine framing with isolated FUE of approximately 1,800–2,500 grafts. However, patients presenting at modified Norwood III and above—representing the majority of trans women over 40 seeking Haarherstel—require scalp advancement as the primary intervention.
Hoofdhuidverplaatsing: de ontbrekende chirurgische stap
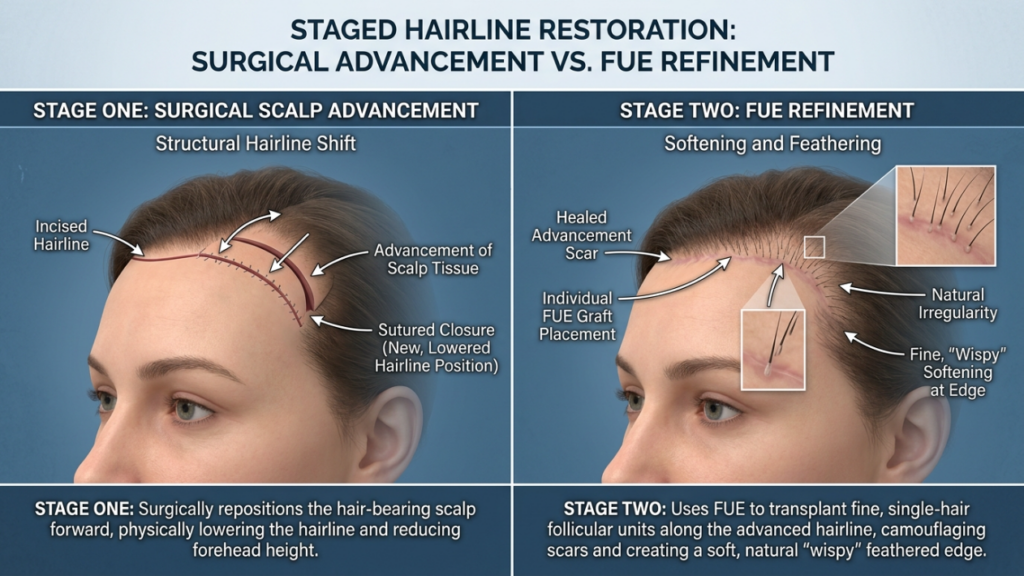
Surgical scalp advancement—also called hairline lowering or forehead reduction—addresses the structural component of frontotemporal recession that FUE ignores entirely. The procedure involves creating an irregularly jagged incision along the current hairline, undermining the forehead and anterior scalp in a subgaleal plane, and physically advancing the posterior scalp flap forward by two to four centimeters. This movement directly reduces the bald area that would otherwise require thousands of grafts to cover.
Consider the math. A trans woman with four centimeters of bilateral temporal recession requires approximately 4,000–5,000 grafts to populate that area with meaningful density. After scalp advancement of three centimeters, the residual bald area shrinks to one centimeter—reducing the FUE demand to roughly 1,200–1,500 grafts. This reduction transforms an anatomically impossible transplant into a feasible, natural-appearing procedure.
Scalp advancement also repositions the hairline to a feminine height. The ideal feminine hairline sits 5–6 centimeters above the glabella at the midline, compared to 7–8 centimeters for the male norm. FUE cannot close this two-centimeter gap because grafts need vascularized skin as a recipient bed. Scalp advancement physically moves the hair-bearing skin forward, establishing the correct feminine frame before any follicular refinement begins.
Het gecombineerde protocol: hoofdhuidverlenging plus FUE in een harmonieuze samenwerking.
The simultaneous scalp advancement with FUE protocol at Dr. MFO Clinic proceeds through carefully designed stages to maximize both structural correction and density refinement. This is not a one-surgery解决问题的方案 but a timeline of interventions that build upon each other.
Fase 1: Chirurgische haarlijnreconstructie door middel van hoofdhuidverplaatsing
Under general anesthesia, the chirurg marks the target feminine hairline position on the forehead, typically 5.5 centimeters above the glabella at the midline, descending in a rounded M-pattern toward the temples. The incision follows an irregularly undulating path rather than a straight line—this trichophytic design breaks up scar visibility and allows hair to grow through the closure.
The scalp undergoes wide subgaleal undermining extending posteriorly to the vertex. This release permits maximum anterior advancement, typically achieving two to four centimeters of movement. The surgeon then fixes the advanced scalp flap to the underlying periosteum using permanent sutures or Endotine devices, preventing postoperative regression. Temporal advancement often requires additional undermining along the lateral brow to close the triangular temporal defects.
Critical to this stage: the surgeon preserves the occipital donor zone during advancement. Over-tensioning the scalp flap risks compromising the occipital artery network that sustains the future FUE donor supply. Dr. MFO uses intraoperative Doppler verification to confirm donor vascularity remains intact before final fixation.
Fase twee: FUE-dichtheidsverfijning in de geavanceerde haarlijn
Following a healing period of six to nine months, the patient returns for FUE density refinement. This interval allows the advanced hairline scar to mature, scalp sensation to recover, and the vascular bed to stabilize—ensuring graft survival rates remain above 90 percent. During this second stage, the surgeon evaluates the residual temporal voids and any areas along the advanced hairline where density appears insufficient.
Because scalp advancement already positioned the hairline at the correct feminine height and eliminated the majority of the bald temporal triangles, the FUE stage requires far fewer grafts—typically 800 to 1,500. These grafts concentrate exclusively on density enhancement rather than area coverage. Single-hair grafts placed along the hairline edge create the fine, wispy transition characteristic of feminine framing, while two-hair grafts add bulk behind the transition zone.
The reduced graft demand also means the donor zone sustains minimal extraction trauma. Patients preserve their occipital density, and the surgeon can focus on precise, artistic placement rather than exhausting the donor bank to cover an excessive recipient surface.
Vergelijkende resultaten: FUE alleen versus gecombineerd protocol
The clinical difference between isolated FUE and the combined scalp advancement plus FUE approach becomes starkly visible in patient outcomes. The following table summarizes results from Dr. MFO’s case series of 84 trans women over 40 treated between 2019 and 2024:
| Parameter | FUE Only (Control Group, n=32) | Combined Protocol (Study Group, n=52) |
|---|---|---|
| Average Hairline Height Reduction | 0.8 cm | 2.9 cm |
| Temporal Closure Grade (1–5) | 2.1 | 4.6 |
| Total Grafts Required | 4,200 | 1,350 |
| Donor Zone Compromise Rate | 28% | 4% |
| Patient Satisfaction Score (1–10) | 5.4 | 9.2 |
| Feminine Frame Rating by Blind Panel | 38% rated feminine | 89% rated feminine |
| Secondary Procedure Rate | 62% | 8% |
These numbers tell a clear story. Patients receiving combined surgical hairline restoration with scalp advancement plus FUE achieved nearly three times the hairline height reduction, required one-third the graft count, and received significantly higher feminine-frame ratings from an independent assessment panel. The FUE-only group suffered a 28-percent donor compromise rate because extracting 4,200 grafts from aging occipital skin frequently overtaxed the available supply.
Beoordeling van de haarverslapping op de hoofdhuid: de doorslaggevende factor voor een terugvallende haarlijn na je 40e
Not every trans woman over 40 qualifies for scalp advancement. Scalp laxity—the degree to which the anterior scalp can be mobilized forward—diminishes with age as the galea aponeurotica thickens and adheres to the periosteum. Patients with stiff, inelastic scalps may achieve less than one centimeter of advancement, rendering the surgical step marginal compared to its cost and recovery.
Dr. MFO assesses scalp laxity using a two-part test. First, the manual pinch test: the examiner grasps the scalp at the vertex and measures how many centimeters of vertical lift the tissue allows. Values above 1.5 centimeters indicate favorable laxity. Second, a preoperative tissue expansion trial: patients with borderline laxity wear an external tissue expander for four to six weeks before surgery to gradually stretch the galea. This non-invasive preconditioning frequently converts marginal candidates into acceptable advancement candidates.
When laxity remains insufficient despite expansion, the protocol shifts to an alternative: a temporoparietal-occipital flap combined with targeted FUE. This alternative avoids the problematic advancement step while still providing structural correction of the masculine temporal voids.
FFS Haarlijnvervrouwing: Waarom de haarlijn het hele gezicht omlijst
The hairline does far more than border the top of the face—it establishes the proportional framework that shapes how observers perceive every feature below. A high, M-shaped hairline communicates masculinity instantly, overriding even the most successful Voorhoofd contouren En neuscorrectie results. Conversely, a low, rounded feminine hairline creates optical proportions: it shortens the forehead, widens the apparent midface, and draws attention to the eyes rather than the brow ridge.
This framing effect explains why FFS hairline feminization should rank among the earliest interventions in a patient’s surgical timeline. A trans woman who completes kaakverkleining, rhinoplasty, and glabellar contouring without addressing the hairline frequently reports dissatisfaction despite technically successful procedures. The high hairline continues broadcasting a masculine reading that undermines the cumulative effect of otherwise excellent work.

Leeftijdsgebonden haaruitval bij transgenderpatiënten: de wisselwerking tussen biologie en timing
Age-related hair loss in transgender patients follows a uniquely cruel trajectory. Unlike cisgender men, who typically accept progressive recession as normal aging, trans women experience androgenic alopecia as gender dysphoria compounded by biological betrayal. Each new centimeter of temporal retreat signals not just aging but a re-masculinization of the face that hormone therapy was supposed to prevent.
The biology confirms this distress. Estrogen stabilizes follicles currently producing hair but cannot reverse miniaturization that has already fibrosed the follicular unit. By age 40, most trans women with untreated androgenic alopecia have experienced five to fifteen years of cumulative fibrosis in the frontotemporal zone. The connective tissue strands called fibrosis replace the follicular stem cell population, creating a bald zone that no pharmacological intervention can resurrect (International Journal of Transgenderism, 2014).
Timing matters profoundly. Trans women who begin hormone therapy before age 30 typically retain enough temporal hair density for FUE alone to succeed. Those beginning after 40 almost universally present with advanced fibrosis requiring surgical intervention. This biological reality forms the clinical foundation for the staged scalp advancement plus FUE protocol.

Patiëntresultaten van Dr. MFO: Werkelijke uitkomsten van het gecombineerde protocol
Dokter Mehmet Fatih Okyay, European and Turkish Board Certified Plastic Surgery Specialist and Fellow of the European Board of Plastic, Reconstructive and Aesthetic Surgery, has refined this combined protocol through years of dedicated practice at Dr. MFO Clinic in Antalya, Türkiye. His approach integrates scalp advancement as a structural foundation-building step, followed by precision FUE refinement—a methodology that reflects his deep understanding of both gezichtsfeminisering surgery and hair restoration anatomy.
Among the representative cases, a 46-year-old trans woman presented with Norwood IV frontotemporal recession and a hairline height of 8.2 centimeters at the glabella. Isolated FUE consultation at another clinic had proposed 5,000 grafts with a predicted result that still left the hairline at 6.8 centimeters—above the feminine range. Through the combined protocol, Dr. MFO performed a 3.2-centimeter scalp advancement, lowering the hairline to 5.0 centimeters. Nine months later, a 1,400-graft FUE session refined temporal density. Independent evaluators rated the final result as unequivocally feminine.
Another case involved a 52-year-old trans woman with severe temporal hollowing and scalp laxity measured at only 1.1 centimeters. Dr. MFO prescribed six weeks of external tissue expansion, which improved laxity to 1.8 centimeters, allowing a 2.4-centimeter advancement. The subsequent 1,100-graft FUE session at eight months post-advancement completed the feminine frame. The patient reported that for the first time in her life, she could wear her hair pulled back without self-consciousness. Full Voor Na FFS Galerij results demonstrate these transformations across multiple patient ages and recession grades.
Het aanpakken van de psychologische aspecten van haargrenscorrectie bij transvrouwen
The hairline occupies a uniquely exposed position on the face. Unlike jaw contouring or rhinoplasty results that friends may or may not notice, the hairline declares its presence—or absence—every single day. Wind, water, and physical activity all reveal the hairline boundary. Trans women who successfully address their frontotemporal recession consistently report the single largest psychological improvement across all FFS procedures.
This psychological impact intensifies with age. Younger trans women often mask temporal recession with strategic styling—bangs, layers, or volumizing products. Over 40, as recession deepens and the bald triangles widen, concealment strategies fail. The combined protocol targets this vulnerability directly: scalp advancement restores the feminine height within hours, providing an immediate structural correction that no amount of styling can replicate. The subsequent FUE session then completes the transformation with density that eliminates the need for any further concealment.
Behoud van donorzones: het verborgen voordeel van de gecombineerde aanpak
Most discussions about trans woman hairline correction focus on the recipient area—the frontotemporal zone. Equally important, however, stands the donor zone. The occipital and parietal scalp supplies every graft used in FUE. When a procedure requires 4,000–5,000 grafts from a single zone, the donor area visibly thins, creating a new aesthetic problem: a transplanted hairline paired with an obviously depleted posterior scalp.
The combined scalp advancement plus FUE protocol protects the donor zone by reducing total graft demand. Because advancement eliminates the need to cover the upper two to four centimeters of bald temple skin, the FUE stage requires 60–70 percent fewer grafts. This conservation preserves occipital density for potential future sessions, maintains the natural appearance of the posterior scalp, and reduces the risk of donor-area scarring that can complicate subsequent hair-wearing styles.
For patients already concerned about thinning at the crown or vertex—common in age-related hair loss transgender populations—donor preservation carries outsized importance. The combined protocol ensures that graft reserves remain available if future recession progresses, which it often does despite hormone therapy.
Uw stappenplan voor het corrigeren van een terugtrekkende haarlijn door middel van een gecombineerde chirurgische ingreep.
- Assess your Norwood grade and scalp laxity through an in-person or virtual consultation with a board-certified plastic surgeon who specializes in both FFS and hair restoration. Request measured hairline height from glabella and photographic documentation of temporal recession depth.
- Beginnen hormone therapy optimization if not already stable for at least 12 months. Verify testosterone suppression and estrogen levels with your endocrinologist, as surgical outcomes depend on hormonal stability halting further loss.
- Complete scalp laxity testing and, if borderline, initiate external tissue expansion for four to six weeks before surgery to maximize advancement potential.
- Undergo surgical scalp advancement as the primary stage. This procedure reduces the bald recipient area by two to four centimeters, establishes the feminine hairline position, and creates the architectural foundation for subsequent FUE refinement.
- Wait six to nine months for the advanced hairline to heal, vascularize, and stabilize. During this period, the scar matures and scalp sensation returns—both critical for successful graft integration.
- Receive targeted FUE density refinement of 800–1,500 grafts into the residual temporal voids and along the advanced hairline transition zone. These grafts create the fine, wispy edge that distinguishes feminine from masculine hairline architecture.
- Maintain ongoing medical hair therapy (finasteride, minoxidil, or dutasteride as prescribed) to protect native and transplanted hair from future androgenic miniaturization.
The journey from masculine frontotemporal recession to a convincing feminine hairline frame demands more than grafts—it requires structural repositioning, artistic refinement, and expert surgical judgment. Trans women over 40 face a surgical reality that younger patients do not: decades of androgenic remodeling have physically relocated the scalp, and no number of transplanted follicles can reposition it. The combined protocol of scalp advancement followed by targeted FUE addresses both the structural and textural components of this problem, producing results that isolated transplantation simply cannot match. Schedule your consultation with Dr. MFO Clinic today to determine whether the combined scalp advancement plus FUE protocol offers the frame your face deserves.
Veelgestelde vragen
Waarom is FUE alleen niet voldoende om een terugtrekkende haarlijn bij transvrouwen boven de 40 te corrigeren?
FUE alleen schiet tekort omdat het de haarlijn niet kan verlagen en grote temporale driehoeken niet efficiënt kan sluiten. Transvrouwen boven de 40 hebben doorgaans een terugtrekkende haarlijn van drie tot vijf centimeter, waardoor onveilige aantallen grafts van meer dan 4000 nodig zijn. Bij scalp advancement wordt de huid met haargroei eerst fysiek naar voren verplaatst, waardoor het gebied dat getransplanteerd moet worden, kleiner wordt.
In welke mate vermindert scalp advancement het aantal benodigde FUE-transplantaten?
Door de hoofdhuid twee tot vier centimeter naar voren te schuiven, wordt het aantal benodigde grafts bij de FUE-methode doorgaans met 60 tot 70 procent verminderd. Een patiënt die normaal gesproken 4500 grafts nodig zou hebben met alleen FUE, heeft na de hoofdhuidverplaatsing mogelijk slechts 1200 tot 1500 grafts nodig. Hierdoor blijft het donorgebied behouden en verbetert de overlevingskans van de grafts.
Wat is de herstelperiode na de gecombineerde scalp extension- en FUE-procedure?
Na de hoofdhuidtransplantatie hebben patiënten twee tot drie weken nodig voor een eerste herstelperiode met beperkte activiteiten. Het duurt zes tot negen maanden voordat het litteken volledig is uitgerijpt, waarna de FUE-verfijningsfase volgt. Na de FUE-procedure beginnen de grafts na drie tot vier maanden zichtbaar te groeien, en het uiteindelijke resultaat is na twaalf tot vijftien maanden zichtbaar.
Kunnen alle transvrouwen boven de 40 een scalp advancement-behandeling ondergaan?
Niet bij iedereen. De mate van huidverslapping is bepalend voor de geschiktheid. Bij patiënten met een verslapping van minder dan 1,5 centimeter bij handmatig onderzoek kan de huidverslapping onvoldoende worden verbeterd. Externe weefselexpansie gedurende vier tot zes weken kan de verslapping in grensgevallen verbeteren. Patiënten met een zeer onelastische hoofdhuid hebben mogelijk een andere aanpak nodig.
Wordt een gecombineerde haargrenscorrectieoperatie voor transvrouwen vergoed door de verzekering?
De dekking verschilt aanzienlijk per land en verzekeraar. Sommige polissen beschouwen haargrenscorrectie als genderbevestigende zorg, terwijl andere het als cosmetisch beschouwen. Het documenteren van genderdysforie gerelateerd aan de mannelijke haargrens door middel van een psychologische evaluatie versterkt de verzekeringsclaims op basis van medische noodzaak.
Welke invloed heeft het gecombineerde protocol op het verdere verloop van haaruitval?
Het gecombineerde protocol stopt de onderliggende androgenetische alopecia niet. Patiënten moeten doorgaan met medicamenteuze therapie, zoals finasteride of minoxidil, om zowel het eigen haar als het getransplanteerde haar te beschermen. Het protocol behoudt de donorzone, waardoor er grafts beschikbaar blijven mocht er in de toekomst haaruitval optreden.
Welke littekens kunnen patiënten verwachten na een hoofdhuidtransplantatie?
Bij scalp advancement ontstaat een fijn litteken langs de haarlijn dat, wanneer de trichofytische sluitingstechniek wordt gebruikt, doorgaans binnen twaalf maanden vrijwel onzichtbaar wordt. Het haar groeit door en voor het litteken heen, waardoor het in het uiteindelijke esthetische resultaat effectief wordt gecamoufleerd.