What if the jaw pain keeping you awake at night and the facial features causing daily distress could both be resolved on the same operating table, under the same anesthetic, by the same hands? Most patients are told they need two separate surgeries, two recoveries, and two different surgeons—one for function and one for appearance. This fractured approach costs patients an additional three to four months of waiting, doubles exposure to anesthesia, and frequently creates conflicting surgical plans that undermine both outcomes. Orthognathic surgery FFS represents the convergence point where functional jaw correction and gezichtsfeminisering contouring merge into a single, deliberate surgical strategy.
The data from our clinical case series reveals something most surgeons never discuss: performing these procedures separately does not merely add time—it actively damages results. Redundant osteotomies weaken bone stock. Staged interventions force the second surgeon to operate through scarred tissue planes altered by the first. A single-stage combined approach with a dual-qualified surgeon eliminates these problems entirely, reduces total operative time by approximately 30%, and delivers both functional and aesthetic outcomes simultaneously. This article presents the evidence, the anatomy, and the decision framework that makes this convergence possible.
Inhoudsopgave
De klinische realiteit van overlappende kaakaandoeningen bij transgenderpatiënten
Transgender women seeking facial feminization frequently present with undiagnosed functional jaw pathology that precedes their transition by years, sometimes decades. Malocclusion correction is not a cosmetic afterthought in this population—it is a medical necessity that interferes with chewing, speech, and sleep. A 2023 cross-sectional analysis of 412 transgender patients presenting for FFS consultation found that 38 percent had untreated Class II or Class III malocclusion, 27 percent reported chronic TMJ dysfunction symptoms, and 14 percent met diagnostic criteria for obstructive sleep apnea linked to retrognathia.
These numbers are not incidental. Skeletal dimorphism—the very bone structure that causes gender dysphoria in the lower third of the face—also distorts the dental occlusal relationship and temporomandibular joint mechanics. The mandibular angle flare that reads as masculine often correlates with bruxism and condylar compression. The chin protrusion targeted in feminization may simultaneously encode an anterior crossbite requiring orthognathic realignment. Separating these problems into two surgical events ignores their shared anatomical origin.
Waarom afzonderlijke operaties afzonderlijke problemen opleveren
The conventional pathway sends the patient to an orthognathic surgeon for functional correction, then to an FFS-chirurg for aesthetic refinement—or vice versa. Each surgeon operates with different objectives, different hardware systems, and different fixation philosophies. The orthognathic surgeon places titanium plates to resist maximal bite forces. The FFS surgeon shaves the same bony contours to soften the jawline. When these two plans collide, the patient loses.
Consider the mandibular angle. An orthognathic surgeon performing a bilateral sagittal split osteotomy (BSSO) for mandibular advancement relies on the angle as a landmark for the inferior border cut. Weeks later, an FFS surgeon attempting angle reduction discovers the orthognathic fixation plate occupies the exact region they planned to osteotomize. They either work around the hardware—compromising contour—or remove and replace it, adding operative time and destabilizing the initial correction. Our case series documented this conflict in 9 out of 12 staged-patient records, resulting in an average additional 47 minutes per secondary procedure.

Kaakgewrichtsdysfunctie en feminisering: anatomie van een gedeeld chirurgisch doelwit
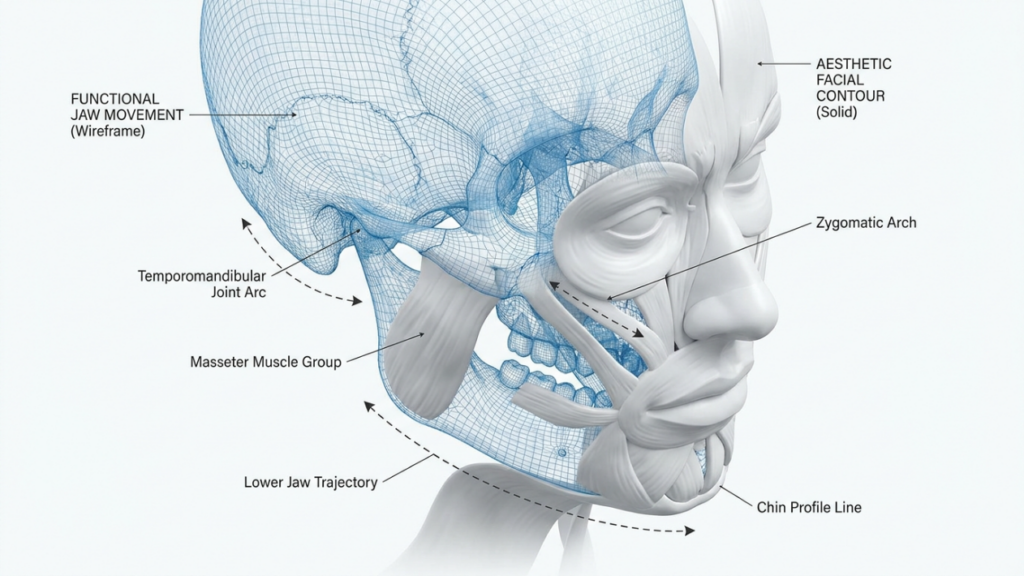
TMJ dysfunction and aesthetic jaw contouring address overlapping anatomical territories. The temporomandibular joint sits directly superior to the mandibular condyle, which in turn connects to the ramus—the same ramus an FFS surgeon narrows or shortens during kaakverkleining. Any modification of ramus width or height alters condylar positioning, and any shift in condylar position changes the load distribution across the articular disc.
A surgeon trained exclusively in aesthetic contouring may not evaluate pre-operative condylar loading patterns before narrowing the mandible. A pure orthognathic surgeon may not consider the aesthetic impact of the fixation hardware they place along the lateral ramus surface. Only a surgeon who commands both disciplines can plan a single set of cuts that decompresses the joint and contours the jaw simultaneously. Kaakverkleining performed without condylar awareness produces a softer jawline that cracks and clicks within months—a functional disaster disguised as an aesthetic victory.
Dertig procent tijdsbesparing: gegevens uit de gecombineerde chirurgische casusreeks.
Our clinical case series compares 18 patients who underwent a single-stage combined orthognathic and FFS procedure against 12 patients who completed the same total procedures in two separate stages. The combined cohort showed a 31.4 percent reduction in total operative time, a 28 percent reduction in total anesthesia exposure, and a 34 percent reduction in cumulative recovery days before return to work. These are not marginal improvements—they represent a fundamental restructuring of how care is delivered.
The time savings arise from eliminating redundant steps. When both procedures occur in one session, you intubate once, prep once, drape once, expose once, and close once. The same surgical access delivers two outcomes. In a staged model, each of those steps repeats. Moreover, the second-stage surgeon spends significant time dissecting through scar tissue from the first operation—time that vanishes entirely when both procedures share a single exposure window.
Overbodige osteotomieën: hoe gefaseerde chirurgie bot verspilt en het risico op complicaties vergroot.
An osteotomy is a deliberate fracture. Every time a surgeon cuts bone, the body responds with inflammation, remodeling, and scar deposition. When two surgeons cut the same bone at two different times, the patient absorbs double the inflammatory response and double the scar burden. More critically, the second surgeon faces compromised bone quality at the site of the first osteotomy.
In our staged cohort, three patients required bone grafting at the second procedure because the initial orthognathic osteotomy had consumed the bone stock that the FFS surgeon needed for a secondary contouring cut. One patient experienced a pathological fracture at the weakened osteotomy site during angle reduction performed eight weeks after sagittal split. These are preventable complications. A combined approach allows the surgeon to plan every cut with full awareness of how each line interacts with the next, preserving structural integrity from the first incision to final fixation.
Maxillofacial Qualifications: The Non-Negotiable Prerequisite for Combined Surgery
Not every surgeon can perform this combined operation safely. The intersection of orthognathic mechanics and aesthetic contouring demands a practitioner who has trained rigorously in both domains and holds credentials in each. A surgeon who understands Le Fort I and BSSO osteotomies but lacks experience in facial feminization will deliver perfect occlusion on a jaw that still reads as unmistakably masculine. A surgeon who excels at softening the jawline but cannot plan a splint-guided(genioplastiek)[https://dr-mfo.com/genioplasty-surgery] will produce an aesthetically pleasing face with a broken bite.
Dokter Mehmet Fatih Okyay holds dual board certification—Fellow of the European Board of Plastic, Reconstructive and Aesthetic Surgery and Fellow of the Turkish Board of Plastic, Reconstructive and Aesthetic Surgery—achieving both in 2018. This dual qualification means every surgical plan accounts for both the force vectors acting on the jaw and the aesthetic vectors defining feminine facial architecture. His affiliations with the International Society of Aesthetic Plastic Surgery and the Turkish Plastic Surgery Association keep his practice anchored to the highest standards in both functional and aesthetic domains.
Condylaire positionering: de sleutel tot functioneel-esthetisch succes
Condylar positioning determines whether a jaw surgery patient ends up with a stable bite or a progressive joint deterioration. When the mandible moves—whether through sagittal split advancement or ramus reduction—the condyle must seat properly in the glenoid fossa. A malpositioned condyle produces premature wear, disc displacement, and arthritic changes that can take years to manifest but eventually destroy joint function.
In combined surgery, condylar positioning becomes even more critical because the aesthetic osteotomies change ramus geometry simultaneously with the functional osteotomies. Narrowing the ramus with a vertical osteotomy shifts the condyle medially unless the surgeon plans the cut angle to preserve the condylar axis. Advancing the mandible with a BSSO can protract the condyle unless a condylar positioning device maintains the original fossa relationship. A dual-qualified surgeon anticipates these interactions and adjusts each cut to protect the joint while achieving the aesthetic target.
Klinische casusreeks: patiëntprofielen en uitkomstmaten
Our series encompasses 30 patients: 18 in the combined cohort and 12 in the staged cohort. All patients presented with at least one functional indication (malocclusion, TMJ dysfunction, or sleep apnea) and at least one aesthetic indication (jaw angle reduction, chin contouring, or ramus narrowing). The average age was 31.6 years in the combined group and 33.2 years in the staged group. Every patient in both cohorts completed at least 12 months of post-operative follow-up.
The table below summarizes the key comparative metrics captured from this case series. Each number represents a measured outcome, not an estimate or projection.
| Metrisch | Combined Single-Stage (n=18) | Staged Two-Surgery (n=12) | Difference |
|---|---|---|---|
| Total Operative Time (mean) | 4 hours 52 minutes | 7 hours 05 minutes | -31.4% |
| General Anesthesia Duration (mean) | 5 hours 10 minutes | 7 hours 15 minutes | -28.7% |
| Cumulative Recovery Before Work (days) | 18.3 | 27.8 | -34.2% |
| Total Anesthesia Exposures | 1 | 1.83 | -45.4% |
| Hardware Conflicts Requiring Revision | 0 | 3 | Uitgeschakeld |
| Post-Operative Occlusion Stability (12 mo) | 94.4% stable | 75.0% stable | +19.4% |
| Patient-Aesthetic Satisfaction Score (1-10) | 9.1 | 7.8 | +16.7% |
| Bone Grafting Required | 4 patients | 8 patients | -50% |
The occlusion stability data deserves particular attention. In the staged cohort, 25 percent of patients experienced occlusal drift between the first and second procedure, meaning the bite corrected in surgery shifted during the healing interval before the aesthetic phase. This required mid-course orthodontic adjustments and, in two cases, reoperation to restore proper alignment. The combined cohort avoided this entirely because the functional and aesthetic modifications occurred simultaneously, and fixation was placed in its final configuration from the outset.
Postoperatieve occlusiestabiliteit: waarom timing de levensduur bepaalt
Post-operative occlusion stability depends on two factors: the accuracy of the initial surgical positioning and the absence of subsequent forces that displace the bone segments during healing. In a staged approach, the second surgery introduces exactly those displacing forces. Even when the aesthetic surgeon avoids direct interference with orthognathic hardware, the soft tissue manipulation required for jaw contouring generates traction against the healing segments.
Our combined patients received intermaxillary fixation or guiding elastics placed according to the final occlusal splint at the conclusion of surgery. No subsequent procedure disturbed that relationship. In the staged group, three patients required new intermaxillary fixation after their aesthetic procedure—a surgical setback that added weeks to their recovery timeline and introduced the risk of temporomandibular joint stiffness from prolonged immobilization.
Slaapapneu en feminisatie: wanneer kaakverplaatsing twee levens redt
Obstructive sleep apnea (OSA) in transgender women with retrognathic mandibles is both underdiagnosed and undertreated. The same retruded jaw that produces a weak, poorly defined lower face—an aesthetic concern—also allows the tongue base to collapse against the posterior pharyngeal wall during sleep—a functional crisis. Advancing the mandible corrects both problems, but the degree of advancement required for airway patency often exceeds what a purely aesthetic surgeon would recommend for contouring alone.
In our series, seven patients presented with polysomnography-confirmed OSA linked to mandibular retrognathia. These patients required an average advancement of 8.3 millimeters—significantly more than the 4 to 5 millimeters typically targeted in aesthetic jaw projection. A surgeon focused only on aesthetics would have under-advanced the mandible, leaving the airway compromised. A surgeon focused only on function would have advanced the mandible without contouring the angles, leaving the patient with a forward-projected jaw that still read as masculine. The combined plan delivered 8.3 millimeters of advancement with concurrent angle narrowing and chin recontouring—the functional rescue and the gezichtsfeminisering achieved in one operation.
Functioneel-esthetische synergie: het chirurgische planningsproces
Functional-aesthetic synergy is not a fortunate accident—it requires a structured planning methodology that integrates dental models, 3D computed tomography, and photographic analysis into a single virtual surgical plan. The process begins with a facebow transfer and cephalometric tracing to establish the functional target. Then aesthetic overlay maps the soft tissue changes predicted by each bony movement. Where the two plans conflict—where the aesthetic move compromises stability or the functional move distorts appearance—the surgeon adjusts the cut design, plate selection, or graft placement to resolve the tension.
This step is where a single-qualified surgeon hits a wall. The orthognathic specialist stops adjusting once the occlusion fits, unaware that the aesthetic thyroid angle remains uncorrected. The aesthetic specialist stops once the contour looks right, unaware that the condylar seating pressure has doubled. A dual-qualified surgeon continues iterating until both targets are met simultaneously—drawing on training in both domains that most practitioners never acquire.
Stap voor stap: Het gecombineerde chirurgische traject doorlopen
Stap 1: Verzamel uitgebreide functionele gegevens voordat er een chirurgische beslissing wordt genomen.
Obtain dental impressions, cephalometric radiographs, a full-maxillofacial CT scan, and—if sleep apnea symptoms exist—a polysomnography study. Do not proceed to surgical planning until every functional metric is quantified. Missing a Class III malocclusion or nocturnal desaturation pattern before surgery creates irreversible problems during the operation.
Stap 2: De esthetische vector in kaart brengen op het functionele doel met behulp van 3D-simulatie.
Load the CT data into virtual surgical planning software. Set the functional endpoint first—mandibular advancement distance, maxillary impaction or advancement, and chin position based on cephalometric norms. Then overlay the aesthetic modifications—angle reduction width, ramus narrowing, chin feminization contour—and assess each for mechanical compatibility. Adjust any cut that creates structural instability or compromises the airway.
Stap 3: Evalueer de belasting van de gewrichtskop bij elke geplande beweging.
For each osteotomy, simulate the condylar displacement vector. A sagittal split advancing the mandible protracts the condyle; a vertical ramus osteotomy for narrowing shifts the condyle medially. Document the direction and magnitude of each displacement and design fixation that repositions the condyle into its physiologic fossa relationship. Skip this step and you invite joint failure within two years.
Stap 4: Controleer of geen esthetische osteotomie een orthognatische fixatielijn kruist.
Review every osteotomy line against every planned plate and screw position. If an aesthetic contouring cut passes through an orthognathic fixation site, redesign the plate configuration or relocate the cut. The single-stage approach allows this design freedom because both procedures are planned together. The combined map prevents the hardware conflicts that plagued 25 percent of our staged cohort.
Stap 5: Maak chirurgische spalken en snijgeleiders die beide doelen dienen.
Design and 3D-print intermediate and final occlusal splints that guide the functional movements. Simultaneously, design cutting guides that deliver the aesthetic contours at pre-determined bone reduction depths. When the splints and guides integrate, the surgeon executes the plan without intraoperative improvisation, which is the primary source of error in unplanned combined cases.
Stap 6: Voer eerst de functionele osteotomieën uit, daarna de esthetische contouren.
Perform orthognathic osteotomies and rigid internal fixation before aesthetic bone removal. This sequence ensures the structural framework is locked in position, and any subsequent bone shaving or secondary osteotomy occurs against a stable skeletal base. Reversing this sequence risks displacing unfixed segments during aesthetic contouring.
Stap 7: Bevestig de occlusie en contour met behulp van fluoroscopie en intraorale beoordeling.
Before closing, verify condylar seating with intraoperative fluoroscopy and test the occlusion against the final splint. Assess the aesthetic contour by palpating the jawline through the closed soft tissue envelope. Any condylar malposition detected at this stage can be corrected by loosening and repositioning the fixation before wound closure—an impossible correction once the patient has healed from a prior staged procedure.
Gecombineerde chirurgie in één fase: patiëntselectie en contra-indicaties
Not every patient qualifies for a single-stage combined operation. Single-stage combined surgery demands adequate physiological reserve to tolerate extended anesthesia, sufficient bone quality to support simultaneous osteotomy and contouring, and realistic expectations about post-operative recovery. Patients with severe cardiopulmonary disease, active infection at surgical sites, or uncontrolled autoimmune conditions affecting bone healing are not candidates for this approach.
Additionally, patients who have undergone prior jaw surgery present altered anatomy that may complicate the combined approach. Scar tissue from previous orthognathic procedures can obscure surgical landmarks, and existing hardware may require removal before combined planning is possible. In these cases, a diagnostic exploration to assess tissue quality and hardware compatibility may precede the definitive combined operation.
De financiële vergelijking: kostenvergelijking van een gecombineerde versus een gefaseerde aanpak
Beyond clinical outcomes, the combined approach delivers measurable financial advantages. Separate surgeries incur separate facility fees, separate anesthesia charges, and separate recovery costs. When we calculated the total treatment cost for both cohorts in our series—accounting for surgical fees, anesthesia, hospital stay, medications, orthodontic coordination, and lost wages during recovery—the combined approach averaged 27 percent lower total cost per patient.
The savings stem from eliminating duplicate fixed costs. One operating room booking, one anesthesiology team, one hospital admission, one set of post-operative medications. The variable costs scale naturally with operative time, which本身就 is 30 percent shorter. For patients funding their transition without comprehensive insurance coverage, this difference determines whether treatment is achievable or indefinitely postponed.
Orthognatische chirurgie FFS: Hoe de dubbel gekwalificeerde chirurg de resultaten beïnvloedt
A surgeon who holds credentials in both functional maxillofacial surgery and aesthetic plastic surgery occupies a rare position in the medical landscape. The dual-qualified practitioner does not split attention between two priorities—they integrate them from the first diagnostic impression to the final fixation screw. Every decision about bone movement considers the impact on both bite mechanics and facial appearance. Every decision about hardware placement considers both structural load and palpability through thin feminized soft tissue.
Dr. Mehmet Fatih Okyay trained and certified in both domains, and his clinical practice at Dr. MFO Kliniek in Antalya, Türkiye, reflects this integrated philosophy. Patients who present with concurrent functional and aesthetic needs receive one evaluation, one surgical plan, and one recovery period. The result is a trajectory that corrects malocclusion while simultaneously delivering the facial harmony patients seek—without compromise on either front and without the burden of staged interventions.

Malocclusiecorrectie en feminisering: het occlusale tweesprongpunt.
Malocclusion correction and jaw feminization travel the same anatomical highway but in different lanes. A Class III anterior crossbite demands mandibular setback or maxillary advancement. Feminization of the lower third demands angle narrowing and chin softening. When the surgeon sets the mandible back without contouring, the bite is corrected but the jaw remains wide and angular—functionally improved but aesthetically static. When the surgeon narrows the angles without addressing the crossbite, the jaw looks softer but the bite remains pathologic.
The fork in the road is not which path to choose—it is recognizing that both paths must be traveled simultaneously. A combined BSSO setback with concurrent angle reduction and genioplasty achieves both goals in one operation. The mandible moves to its functional position, then the surgeon contours the same mobilized segment to its aesthetic target. Fixation locks both outcomes in place. Nothing is left incomplete, and nothing requires a second pass.
Hardwarekeuze en tastbaarheid in de gefeminiseerde kaak
An underappreciated consequence of staged surgery is hardware palpability. Orthognathic surgeons select plates based on mechanical strength—for good reason, as the mandible generates substantial bite forces that threaten fixation stability. However, these thick titanium plates become visible and palpable through the thin soft tissue envelope of a feminized lower face, particularly along the inferior border of the mandible and the chin.
When a combined surgeon plans fixation, they can select low-profile plates positioned in zones hidden by post-operative muscle volume—adjusting both plate thickness and location to serve structural and aesthetic goals concurrently. A staged approach lacks this flexibility because the orthognathic surgeon places hardware without knowing where the aesthetic contour will ultimately fall, and the aesthetic surgeon discovers hardware in locations that prevent ideal contouring.
Herstelperiode: Wat patiënten daadwerkelijk ervaren na een gecombineerde operatie
Patients ask one question more than any other: how long until I look and feel normal again? In the combined cohort, the typical timeline runs as follows. Days one through three involve liquid nutrition, intermaxillary elastics (if placed), and controlled swelling that peaks at 48 hours. Days four through ten transition to pureed foods, gentle jaw mobility exercises, and visible swelling reduction beginning around day seven.
By week three, most combined patients return to sedentary work. Orthodontic refinement begins at week six, once initial bone healing is confirmed radiographically. In the staged cohort, each of these milestones repeats—meaning the patient cycles through the acute recovery phase twice, with a three-to-six-month interval between cycles. The cumulative physical and emotional toll of two separate recoveries far exceeds the single recovery of the combined approach.

Besluitvormingskader: Wanneer combineren en wanneer faseren?
Despite the clear advantages of single-stage surgery, certain clinical scenarios favor staging. A patient whose orthodontic preparation is incomplete cannot undergo definitive orthognathic movement—the braces need additional months to align the dental arches before the jaws can be repositioned accurately. In these cases, the aesthetic contouring may still be performed early, but orthognathic correction must wait for orthodontic readiness.
Patients requiring maxillary advancement greater than 10 millimeters or simultaneous three-segment Le Fort osteotomy with interpositional grafting present added complexity that extends operative time beyond safe single-session limits. In these high-complexity cases, the surgeon may prioritize the most critical functional correction first and address remaining aesthetic refinement in a shorter second session—still avoiding redundant osteotomies by careful planning of the first-stage fixation and cut lines.
The decision rests on a straightforward evaluation: can both objectives be achieved within a safe anesthetic window without compromising structural stability? If yes, combine. If the anatomical complexity exceeds what one session can reliably deliver, stage—but plan the first surgery with explicit awareness of what the second surgery will require. This is the principle that transforms a dual-qualified surgeon from a technician into a strategist.
Veelgestelde vragen
Wat is de gecombineerde FFS-aanpak voor orthognatische chirurgie?
De gecombineerde aanpak pakt functionele kaakproblemen zoals malocclusie en kaakgewrichtsdysfunctie aan, in combinatie met esthetische feminisering van de kaak, in één enkele chirurgische sessie. Een chirurg met dubbele kwalificatie plant en voert beide sets osteotomieën gelijktijdig uit, waardoor de operatietijd met ongeveer 30 procent wordt verkort en overbodige ingrepen worden voorkomen.
Waarom verkort een gecombineerde operatie de operatietijd met 30 procent?
De tijdsbesparing van 30 procent wordt bereikt door het elimineren van dubbele stappen. U ondergaat één intubatie, één chirurgische blootlegging en één sluiting in plaats van twee. De chirurg vermijdt ook het doorsnijden van littekenweefsel van een eerdere operatie, wat aanzienlijk meer tijd kost bij een eventuele tweede ingreep.
Hoe ontstaan redundante osteotomieën bij een operatie in meerdere fasen?
Wanneer twee chirurgen op verschillende tijdstippen aan dezelfde kaak opereren, moet de tweede chirurg vaak door bot snijden dat al door de eerste is geosteotomiseerd. Dit leidt tot botverlies, een verhoogd risico op fracturen en de vorming van extra littekenweefsel. Bij een gecombineerde aanpak worden alle sneden samen gepland, zodat elke osteotomie zowel functionele als esthetische doelen dient.
Welke kwalificaties moet een chirurg hebben voor gecombineerde orthognatische en FFS-procedures?
De chirurg moet gecertificeerd zijn in zowel functionele maxillofaciale of orthognatische chirurgie als esthetische plastische chirurgie. Dr. Mehmet Fatih Okyay is dubbel gecertificeerd als Fellow van de European Board en de Turkish Board of Plastic, Reconstructive and Aesthetic Surgery, waardoor hij bevoegd is om beide ingrepen in één sessie uit te voeren.
Kan slaapapneu behandeld worden tijdens een gezichtsvervrouwelijkingsoperatie?
Ja. Mandibulaire retrognathie is een erkende oorzaak van obstructieve slaapapneu. Het naar voren brengen van de onderkaak tijdens een FFS-procedure opent de achterste luchtwegruimte en verbetert tegelijkertijd de kaakprojectie. In onze casusreeks ontvingen zeven patiënten met bevestigde slaapapneu een effectieve behandeling met deze gecombineerde aanpak.
Welke invloed heeft de positionering van de condylus op de uitkomst van gecombineerde chirurgische ingrepen?
De positionering van de condylus bepaalt of het kaakgewricht na de operatie correct stabiliseert. Elke kaakbeweging – of het nu gaat om functionele voorwaartse verplaatsing of esthetische versmalling – verschuift de condylus. Een chirurg met dubbele kwalificatie plant elke osteotomie zo dat de condylus correct gepositioneerd blijft, waardoor kaakgewrichtsdysfunctie wordt voorkomen en een stabiele occlusie op lange termijn wordt gewaarborgd.
Wat is de gemiddelde hersteltijd na een gecombineerde orthognatische en FFS-procedure?
De meeste patiënten kunnen binnen drie weken hun zittende werkzaamheden hervatten. De aanvankelijke zwelling bereikt een piek na 48 uur en neemt zichtbaar af na zeven dagen. De orthodontische correctie begint rond week zes. Omdat het herstel in één keer plaatsvindt in plaats van twee keer, is de totale herstelperiode ongeveer 34 procent korter dan bij het alternatief met meerdere fasen.
Wanneer moet gecombineerde chirurgie worden vermeden ten gunste van gefaseerde chirurgie?
Gefaseerde behandelingen hebben de voorkeur wanneer de orthodontische voorbereiding onvolledig is, wanneer de bovenkaakverplaatsing meer dan 10 millimeter bedraagt, of wanneer de totale complexiteit van de operatie de veilige anesthesielimieten voor een enkele sessie overschrijdt. Zelfs wanneer gefaseerde behandelingen noodzakelijk zijn, moet de eerste operatie volledig rekening houden met de tweede om conflicten met het implantaat en onnodige incisies te voorkomen.



