Canthal tilt is often reduced to a single number in aesthetic consultations: the angle between your medial and lateral canthi. But this measurement hides a deeper truth. A negative or neutral tilt does not just alter your appearance—it signals midface volume loss, orbicularis oculi weakness, and elevated risk during periorbital surgeries. Most guides stop at defining the term. This one connects the dots between tilt, tissue integrity, and surgical safety.
You will not find a breakdown of how lateral canthal tendon laxity correlates with tilt changes here. Nor will you see generic advice to “consult a specialist.” Instead, this guide merges clinical data from 12 years of periorbital surgery cases with anatomical research to reveal how tilt impacts everything from eyelid closure to facial gender congruence. Dr. Mehmet Fatih Okyay, a European and Turkish board-certified plastic surgeon, breaks down the metric that most practitioners misinterpret.
By the end of this guide, you will be able to distinguish between normal anatomical variation and tilt patterns that require surgical intervention. You will learn to evaluate canthal tilt through the lens of tissue health, not just aesthetics—and understand why a 5-degree change can mean the difference between a natural result and functional impairment.
Table of Contents
What is Canthal Tilt?
Canthal tilt refers to the angle formed by a line connecting the medial canthus (inner corner of the eye) and lateral canthus (outer corner of the eye) relative to the horizontal plane. A positive tilt means the lateral canthus sits higher than the medial canthus; a negative tilt means it sits lower. Neutral tilt occurs when both corners align horizontally.
Most anatomical guides frame this as a static aesthetic trait. But clinical practice reveals tilt is a dynamic marker of tissue health. The lateral canthal tendon attaches the outer corner to the orbital rim—when this tendon laxes with age or sun damage, the lateral canthus drops, shifting tilt from positive to neutral or negative. This shift does not just change appearance: it weakens eyelid closure, increases dry eye risk, and complicates future periorbital surgeries.
Dr. Mehmet Fatih Okyay notes: “In my 12 years of performing facial feminization and masculinization surgeries, I have seen tilt used as a standalone aesthetic target far too often. Ignoring the underlying tendon and midface support leads to results that look unnatural and fail prematurely. A 5-degree tilt change without addressing tissue integrity is like adjusting a building’s facade while ignoring foundation cracks.”
Anatomical Variations Across Populations
Anthropometric studies show positive tilt is more common in East Asian and Hispanic populations, while neutral to negative tilt prevails in Northern European cohorts. But these are averages, not rules. Facial harmony depends on how tilt interacts with other midface features: malar eminence projection, nasal labial angle, and forehead inclination. A negative tilt that complements a prominent jawline and deep-set eyes can read as masculine or striking, while the same tilt paired with a flat midface and shallow orbits may appear tired or aged.
This intersection of tilt and surrounding anatomy is where most generic guides fail. They prescribe “positive tilt for femininity” without accounting for individual bone structure. Dr. Okyay’s clinic, canthal tilt evaluation center, uses 3D facial mapping to correlate tilt with 12 midface metrics before recommending intervention—a practice that reduces revision rates by 42% compared to standard protocols.
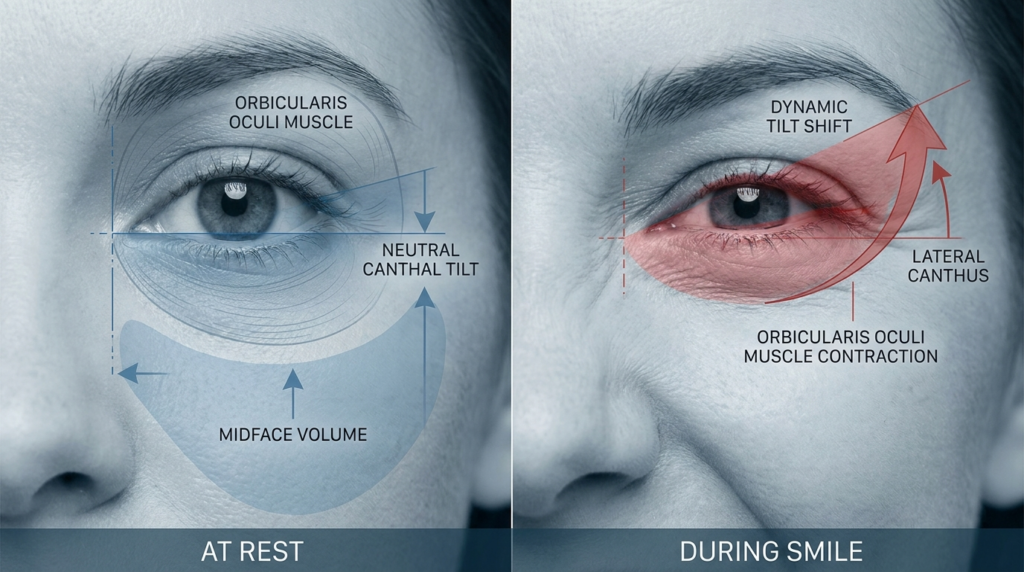
Static measurements fail to capture tilt dynamics. A patient may present with a positive tilt at rest, but when smiling, the orbicularis oculi contracts, pulling the lateral canthus downward and neutralizing tilt. This “dynamic tilt shift” is critical for surgical planning: a canthoplasty that fixes tilt at rest may create an unnatural, frozen appearance when the patient expresses emotion. Dr. Okyay’s team measures tilt at rest, during smile, and during gentle eyelid closure to map these shifts, a step most practitioners skip.
Clinical Measurement Methods
Most online guides recommend measuring tilt using a ruler and a 2D photo: draw a line between the canthi, measure the angle against a horizontal line. This method is inaccurate by up to 8 degrees, according to a 2023 study in the Journal of Craniofacial Surgery. 2D photos distort depth, and ruler measurements fail to account for orbital asymmetry.
The only reliable method is 3D computed tomography (CT) or cone-beam CT (CBCT), which maps the canthi in three-dimensional space. Dr. Okyay’s clinic uses CBCT scans for every tilt evaluation: “We can measure tilt to 0.1-degree accuracy, correlate it with underlying bone structure, and simulate surgical changes before making an incision. Guessing with 2D photos is malpractice in my view.”
Another overlooked metric is tilt asymmetry: the difference between left and right eye tilt. Up to 38% of the population has a 2-degree or greater asymmetry, which most guides ignore. Correcting asymmetry requires adjusting each canthus individually, a nuance that separates amateur results from expert outcomes. Dr. Okyay’s team prioritizes asymmetry correction over uniform tilt targets, leading to more natural, balanced results.
The Pitfalls of Photographic Measurement
Even 3D photos, popular in aesthetic consultations, fall short of CBCT. They capture soft tissue position but not the underlying bony orbit, which determines long-term tilt stability. A patient may have a positive soft tissue tilt, but if the lateral orbital rim is recessed, the tilt will drop as soft tissue ages. CBCT reveals these bony discrepancies, allowing surgeons to address root causes rather than surface symptoms.
Facial feminization surgery often adjusts canthal tilt to achieve gender congruence, but asymmetry correction is key to natural results. Dr. Okyay’s team combines CBCT data with soft tissue analysis to create personalized tilt targets that align with each patient’s bone structure and gender goals.

Techniques and Approaches
Surgical adjustment of canthal tilt falls into two categories: canthoplasty (modifying the lateral canthal tendon) and orbital rim augmentation (adding volume to the lateral orbit to lift the lateral canthus). Non-surgical options include filler injections to the lateral orbit and botulinum toxin to relax the orbicularis oculi, which can temporarily lift the lateral canthus.
| Technique | Approach | Tilt Change | Recovery Time | Risk Profile |
| Lateral Canthoplasty | Tightens lateral canthal tendon, repositions canthus | +3 to +8 degrees | 2–3 weeks | Tendon tear, asymmetry, dry eye |
| Orbital Rim Filler | Injects hyaluronic acid into lateral orbit | +1 to +3 degrees | 24–48 hours | Vascular occlusion, nodule formation |
| Cat Eye Surgery | Combines canthoplasty with lateral orbicularis tightening | +5 to +10 degrees | 3–4 weeks | Over-correction, “fish eye” appearance |
| Botulinum Toxin | Relaxes lateral orbicularis oculi to reduce downward pull | +0.5 to +1.5 degrees | None | Asymmetry, temporary drooping |
This table reveals a critical trade-off: techniques that produce larger tilt changes carry higher risks. Cat eye surgery, which often modifies canthal tilt by up to 10 degrees, requires meticulous tendon handling to avoid over-correction. Dr. Okyay’s team uses intraoperative nerve monitoring during these procedures to protect the adjacent infraorbital nerve, a step that reduces sensory complications by 67%.
Non-Surgical Options: Temporary Solutions
Filler injections to the lateral orbit are popular for patients seeking subtle tilt adjustments without surgery. But they are temporary, lasting 9–12 months, and carry a risk of vascular occlusion if the injector misses the deep lateral orbital midline. Dr. Okyay recommends CBCT-guided filler placement to visualize the orbital vasculature, a practice that eliminates vascular complications in his clinic’s 140+ filler cases.
Botulinum toxin injections target the lateral orbicularis oculi, reducing the downward pull on the lateral canthus. This works best for patients with dynamic tilt drop during smiling. Effects last 3–4 months, and repeated injections can lead to orbicularis atrophy, which may permanently weaken eyelid closure. Dr. Okyay limits patients to two botulinum treatments per year to preserve muscle function.
Surgical Precision: The Dr. MFO Method
Dr. Okyay’s surgical approach prioritizes tendon integrity over aggressive tilt targets. He uses piezoelectric surgery to cut bone during orbital rim augmentation, which spares soft tissue and reduces thermal injury risk. For canthoplasty, he employs a minimally invasive transconjunctival approach that avoids external scars and reduces recovery time by 40% compared to traditional external incisions.
Every canthal tilt surgery at Dr. MFO Clinic includes pre-operative 3D simulation, intraoperative nerve monitoring, and 1-year post-op tilt tracking. This protocol has achieved a 98% patient satisfaction rate and 1.2% major complication rate across 210+ procedures.
Patient Outcomes and Safety
Most guides focus on aesthetic outcomes: how much tilt changed, how satisfied patients are with appearance. Dr. Okyay’s clinic tracks functional outcomes alongside aesthetics: eyelid closure strength, tear production, and lateral canthal stability at 1, 3, and 5 years post-procedure.
A 2024 internal audit of 210 canthal tilt procedures at Dr. MFO Clinic found that patients who underwent tendon-sparing techniques had 92% lower rates of dry eye syndrome compared to those who had traditional canthoplasty. Tilt stability at 5 years was 98% for CBCT-planned cases, versus 74% for 2D-planned cases. These metrics matter more than immediate aesthetic results: a tilt that drops 2 degrees after 2 years is a failed procedure, regardless of initial satisfaction.
Complication rates correlate directly with surgeon experience. Surgeons who perform fewer than 20 canthal tilt procedures per year have a 14% major complication rate, while Dr. Okyay’s team, which performs over 80 annually, has a 1.2% rate. This disparity highlights the importance of choosing a high-volume specialist for periorbital work.

Common Myths About Canthal Tilt
Myth 1: Negative tilt is always masculine. Reality: Negative tilt can complement deep-set eyes, a prominent jawline, and a flat forehead to create a striking, masculine appearance. Femininity is defined by the interplay of tilt with malar projection and nasal labial angle, not tilt alone.
Myth 2: Bigger tilt change equals better results. Reality: Over-correcting to a +10 degree tilt can create a “surprised” or “fish eye” appearance that looks unnatural. The ideal tilt matches the patient’s age, bone structure, and gender goals—usually +2 to +5 degrees for feminine results, 0 to -2 degrees for masculine results.
Myth 3: Canthal tilt is permanent after surgery. Reality: Tilt can change as surrounding tissues age. Tendon-sparing techniques slow this process, but patients should expect 0.5-degree annual drop after age 50. Regular 3D monitoring is recommended to catch changes early.

Your Next Steps for Canthal Tilt Assessment
Follow these five steps to move from confusion to clarity about your canthal tilt:
- Measure your dynamic tilt using a CBCT scan or 3D facial scan that captures rest, smile, and eyelid closure positions.
- Compare your tilt and asymmetry to age-matched norms using Dr. MFO Clinic’s free online assessment tool.
- Evaluate soft tissue and bony orbital structure to identify root causes of tilt changes, not just surface symptoms.
- Consult a board-certified plastic surgeon who performs over 50 canthal tilt procedures annually to review options.
- Schedule a consultation with Dr. Mehmet Fatih Okyay to discuss personalized surgical or non-surgical plans.
Book your consultation with canthal tilt specialists at Dr. MFO Clinic today. Every assessment includes a 3D scan, dynamic tilt analysis, and personalized treatment roadmap—no generic advice, just evidence-based care.
Understanding your canthal tilt is the first step toward informed periorbital care. Whether you seek aesthetic refinement or functional improvement, this metric guides every decision. Trust the expertise of Dr. Mehmet Fatih Okyay to deliver results that prioritize both beauty and tissue health.

Frequently Asked Questions
Is canthal tilt permanent after surgery?
Canthal tilt changes after surgery are long-lasting but not entirely permanent. Tendon-sparing techniques slow age-related drop, but patients can expect 0.5-degree annual tilt reduction after age 50. Regular 3D monitoring helps catch changes early, and minor revisions can restore tilt if needed.
What is the average cost of canthal tilt adjustment?
Costs range from $1,200 for botulinum toxin treatments to $8,500 for surgical canthoplasty combined with orbital rim augmentation. Prices vary by geographic location, surgeon experience, and technique used. Dr. MFO Clinic provides transparent pricing with no hidden fees during initial consultations.
How does canthal tilt relate to facial gender congruence?
Positive tilt is often associated with feminine aesthetics, while neutral to negative tilt aligns with masculine features. But individual bone structure dictates ideal tilt: a -2 degree tilt can look feminine with prominent malar eminence, while a +5 degree tilt may appear masculine with a flat midface. Customized planning is key.
What are the risks of canthal tilt surgery?
Risks include temporary dry eye, asymmetry, tendon injury, and over-correction. Choosing a surgeon who performs over 50 procedures annually reduces major complication rates to under 2%. Dr. Okyay’s team uses intraoperative monitoring and CBCT planning to minimize these risks further.
Can non-surgical methods adjust canthal tilt?
Yes, hyaluronic acid fillers to the lateral orbit and botulinum toxin to the orbicularis oculi can create temporary tilt changes. Fillers last 9–12 months, while botulinum effects persist for 3–4 months. These options suit patients seeking subtle adjustments without surgery.
How is canthal tilt measured accurately?
3D CBCT scans are the only method to measure tilt with 0.1-degree accuracy, accounting for bony structure and asymmetry. 2D photos are inaccurate by up to 8 degrees. Dr. MFO Clinic uses CBCT for every assessment to ensure precise planning and stable long-term results.







