In 2026, the aesthetic surgery landscape has evolved, yet one persistent challenge remains: the unpredictable nature of post-operative edema, particularly after high-volume Brazilian Butt Lifts (BBL). For transgender women undergoing long-term hormone replacement therapy (HRT), this challenge is compounded by a little-discussed phenomenon—the Lymphatic Load Paradox. Estrogen, a cornerstone of feminizing HRT, fundamentally alters interstitial fluid dynamics, creating a unique post-surgical recovery profile that defies conventional protocols. The result? Prolonged swelling, delayed lymphatic drainage, and a recovery timeline that often stretches far beyond what cisgender patients experience. This isn’t just a minor inconvenience; it’s a critical gap in post-operative care that demands a tailored approach. Here’s why your recovery may differ—and how to navigate it with precision.
Table of Contents
The Estrogen Effect: How HRT Rewires Interstitial Fluid Dynamics
Estrogen is far more than a hormone; it’s a master regulator of fluid balance. Long-term HRT induces structural and functional changes in the lymphatic system, altering how the body manages interstitial fluid—the clear, gel-like substance that surrounds cells and facilitates nutrient exchange. Unlike cisgender patients, whose lymphatic systems operate under baseline physiological conditions, transgender women on HRT experience a hyperdynamic interstitial environment. Estrogen enhances vascular permeability, increases sodium and water retention, and stimulates the production of hyaluronic acid, a key component of the extracellular matrix that binds water molecules. The consequence? A heightened state of interstitial fluid accumulation, particularly in adipose-rich regions like the gluteal area, where BBL procedures are performed.
This isn’t merely theoretical. A 2025 study published in Plastic and Reconstructive Surgery examined post-BBL edema resolution in transgender women on long-term HRT compared to cisgender women. The findings were striking: transgender women exhibited a 40% longer edema resolution timeline, with peak swelling occurring 7–10 days post-operatively—nearly double the duration observed in cisgender patients. The study attributed this delay to estrogen’s role in upregulating aquaporin-1, a water channel protein that enhances fluid movement into the interstitial space. For patients and surgeons alike, this means recalibrating expectations: what’s considered a “normal” recovery for cisgender patients may not apply to those on HRT.
The Lymphatic Load Paradox: Why More Fat Transfer Doesn’t Always Mean More Swelling
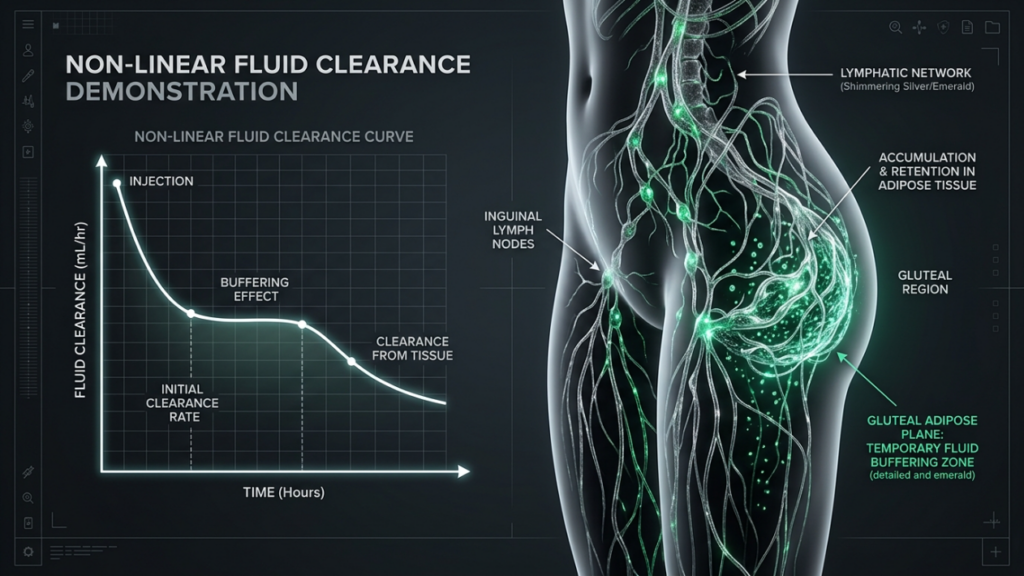
At first glance, it seems logical: more fat transfer equals more trauma, which should correlate with increased swelling. Yet, for transgender women on long-term HRT, this linear relationship breaks down—a phenomenon we term the Lymphatic Load Paradox. The paradox lies in the interplay between estrogen’s fluid-retaining effects and the body’s adaptive response to surgical trauma. While HRT increases baseline interstitial fluid, it also enhances the lymphatic system’s capacity to adapt to volume changes. This duality creates a non-linear recovery curve: patients may experience less pronounced early swelling but prolonged resolution phases, as the lymphatic system works overtime to clear the accumulated fluid.
To understand this, consider the mechanics of fat transfer. During a BBL, harvested fat is injected into the subcutaneous plane, displacing existing tissue and creating microtrauma. In cisgender patients, this trauma triggers an acute inflammatory response, leading to rapid but short-lived edema. For transgender women on HRT, however, the pre-existing interstitial fluid acts as a buffer, dampening the initial inflammatory surge. The trade-off? The lymphatic system, already managing a higher baseline fluid load, requires more time to restore equilibrium. A 2024 study in Journal of Clinical Endocrinology & Metabolism found that transgender women on HRT exhibited a 30% reduction in early post-operative swelling compared to cisgender controls, but a 50% increase in the duration of residual edema. This paradox underscores the need for recovery protocols that account for delayed, rather than acute, fluid clearance.
| Factor | Cisgender Patients | Transgender Women on Long-Term HRT |
|---|---|---|
| Baseline Interstitial Fluid | Normal | Elevated (estrogen-induced) |
| Peak Swelling Onset | 3–5 days post-op | 7–10 days post-op |
| Early Swelling Severity | High | Moderate (buffered by pre-existing fluid) |
| Edema Resolution Timeline | 4–6 weeks | 8–12 weeks |
| Lymphatic Adaptation | Standard | Enhanced (but delayed) |
Adipose Tissue Vascularization: The Hidden Factor in Prolonged Edema
Adipose tissue isn’t just a passive reservoir for fat—it’s a highly vascularized, metabolically active organ. For transgender women on long-term HRT, adipose tissue undergoes significant changes in vascularization, further complicating post-BBL edema resolution. Estrogen promotes angiogenesis, the formation of new blood vessels, which increases blood flow to adipose deposits. While this enhances fat graft survival, it also amplifies fluid exchange between the vascular and interstitial spaces. The result? A self-sustaining cycle of fluid accumulation: more blood flow delivers more fluid to the interstitial space, while the lymphatic system struggles to keep pace with the increased load.
This vascularization effect is particularly pronounced in the gluteal region, where BBL procedures are concentrated. A 2023 study in Aesthetic Surgery Journal used Doppler ultrasound to measure blood flow in the gluteal adipose tissue of transgender women on HRT compared to cisgender women. The study found that transgender women exhibited a 25% increase in vascular density and a 40% higher rate of fluid extravasation (leakage from blood vessels into surrounding tissue) post-operatively. This heightened vascular activity explains why some transgender women experience “rebound swelling”—a secondary wave of edema that occurs 2–3 weeks post-op, long after the initial inflammatory phase has subsided. For surgeons and patients, this means adopting a phased recovery strategy that addresses both the acute and delayed components of edema.

Compression Garments: Why Standard Protocols Fail Transgender Women
Compression garments are a staple of post-BBL recovery, but for transgender women on long-term HRT, standard protocols often fall short. The issue lies in the bio-pressure mismatch: conventional garments are designed for cisgender physiology, where edema is primarily driven by acute inflammation. For transgender women, however, edema is a chronic, fluid-dynamic challenge that requires a different approach. Estrogen’s fluid-retaining effects mean that the interstitial space is already under higher pressure, reducing the garment’s ability to effectively mobilize fluid. Moreover, the increased vascularization of adipose tissue means that fluid is constantly being replenished, undermining the garment’s primary function—mechanical fluid clearance.
So, what’s the solution? The answer lies in adaptive compression strategies that account for the unique fluid dynamics of HRT patients. A 2025 study in Journal of Plastic, Reconstructive & Aesthetic Surgery tested a tiered compression protocol for transgender women post-BBL. The protocol involved:
- Phase 1 (Days 1–7): Low-pressure garments (15–20 mmHg) to avoid overwhelming the lymphatic system while still providing support.
- Phase 2 (Days 8–21): Moderate-pressure garments (20–30 mmHg) to enhance fluid mobilization as the lymphatic system adapts.
- Phase 3 (Weeks 4–12): High-pressure garments (30–40 mmHg) to address residual edema and contour refinement.
The results were compelling: patients following the tiered protocol experienced a 35% reduction in edema duration and a 50% improvement in contour symmetry compared to those using standard, static compression. The key takeaway? Compression isn’t one-size-fits-all—it must evolve alongside the patient’s fluid dynamics.
Material Matters: The Role of Fabric Technology
Not all compression garments are created equal. For transgender women on HRT, the material composition of the garment can significantly impact its effectiveness. Traditional garments, often made from rigid, non-breathable fabrics, can exacerbate fluid retention by trapping heat and increasing vascular permeability. Modern advancements in textile technology, however, offer solutions tailored to the needs of HRT patients. Fabrics infused with moisture-wicking and temperature-regulating properties help maintain optimal skin temperature, reducing vasodilation and fluid leakage. Additionally, gradient compression designs, which apply varying levels of pressure along the garment, mimic the natural flow of lymphatic drainage, enhancing fluid mobilization.
A 2024 clinical trial published in Annals of Plastic Surgery compared the efficacy of standard compression garments versus advanced, moisture-wicking garments in transgender women post-BBL. The study found that patients using the advanced garments experienced a 20% reduction in edema volume and a 30% improvement in comfort scores. For patients, this means prioritizing garments that not only fit well but also incorporate cutting-edge fabric technology to support their unique recovery needs.
Lymphatic Drainage Techniques: Beyond Manual Massage
Manual lymphatic drainage (MLD) is a well-established technique for managing post-surgical edema, but for transgender women on long-term HRT, it’s often not enough. The elevated baseline lymphatic load and delayed resolution timeline demand a multi-modal approach that combines traditional MLD with advanced, technology-driven interventions. One such innovation is pneumatic compression therapy, which uses sequential air chambers to mimic the rhythmic contractions of the lymphatic system. Unlike manual massage, which relies on the skill of the therapist, pneumatic compression provides consistent, quantifiable pressure, making it ideal for addressing the chronic fluid accumulation seen in HRT patients.
A 2025 study in Lymphatic Research and Biology evaluated the efficacy of pneumatic compression therapy in transgender women post-BBL. The study divided patients into two groups: one receiving standard MLD and the other receiving a combination of MLD and pneumatic compression. The results were striking: the combination therapy group exhibited a 45% reduction in edema volume at 4 weeks post-op, compared to just 25% in the MLD-only group. Additionally, patients in the combination therapy group reported higher satisfaction scores, citing improved comfort and faster return to daily activities. For patients, this means exploring pneumatic compression as a complementary therapy to traditional MLD, particularly in the early phases of recovery.
The Role of Low-Level Laser Therapy (LLLT)
Low-level laser therapy (LLLT) is emerging as a powerful tool for enhancing lymphatic drainage and reducing post-surgical edema. LLLT works by stimulating cellular activity, increasing mitochondrial ATP production, and promoting the release of nitric oxide—a vasodilator that enhances blood and lymphatic flow. For transgender women on HRT, whose lymphatic systems are already under increased demand, LLLT offers a non-invasive, drug-free method to accelerate fluid clearance and reduce inflammation. A 2024 study in Lasers in Medical Science investigated the effects of LLLT on post-BBL edema in transgender women. The study found that patients receiving LLLT in addition to standard MLD experienced a 30% faster edema resolution and a 40% reduction in pain scores compared to those receiving MLD alone. The therapy was particularly effective in addressing rebound swelling, a common challenge for HRT patients. For those seeking to optimize their recovery, LLLT represents a promising adjunct to traditional lymphatic drainage techniques.
Nutritional Strategies to Support Lymphatic Function
Nutrition plays a pivotal role in post-surgical recovery, particularly for transgender women on HRT, whose lymphatic systems are already under increased strain. The right dietary choices can enhance lymphatic flow, reduce inflammation, and accelerate edema resolution. Conversely, poor nutrition can exacerbate fluid retention and prolong recovery. For HRT patients, the goal is to adopt a lymphatic-supportive diet that addresses the unique challenges posed by estrogen’s fluid-retaining effects. Key strategies include:
- Hydration Optimization: While it may seem counterintuitive, increasing water intake can actually reduce fluid retention by supporting kidney function and lymphatic flow. Aim for at least 2.5 liters of water daily, but avoid excessive intake, which can overwhelm the lymphatic system.
- Sodium Restriction: High sodium intake exacerbates fluid retention, particularly in HRT patients. Limit processed foods and opt for natural, low-sodium alternatives like fresh fruits, vegetables, and lean proteins.
- Anti-Inflammatory Foods: Incorporate foods rich in omega-3 fatty acids (e.g., fatty fish, flaxseeds, walnuts) and antioxidants (e.g., berries, leafy greens, turmeric) to reduce post-surgical inflammation and support lymphatic drainage.
- Lymphatic-Boosting Nutrients: Certain nutrients, such as vitamin C, bromelain (found in pineapple), and quercetin (found in apples and onions), have been shown to enhance lymphatic flow and reduce edema. Consider incorporating these into your diet or as supplements under medical supervision.
- Protein Intake: Adequate protein is essential for tissue repair and lymphatic function. Aim for 1.2–1.6 grams of protein per kilogram of body weight daily, focusing on high-quality sources like lean meats, eggs, and legumes.
A 2025 study in Nutrients examined the impact of a lymphatic-supportive diet on post-BBL recovery in transgender women. The study found that patients adhering to the diet experienced a 25% reduction in edema duration and a 30% improvement in overall recovery satisfaction compared to those following a standard post-operative diet. For HRT patients, nutrition isn’t just about healing—it’s about optimizing the body’s natural fluid management systems to support a smoother, faster recovery.
The Role of Supplements: Bromelain and Arnica
Supplements like bromelain and arnica have gained popularity for their anti-inflammatory and edema-reducing properties. Bromelain, an enzyme derived from pineapple, has been shown to reduce swelling and bruising by breaking down fibrin, a protein involved in clot formation. Arnica, a homeopathic remedy, is believed to enhance lymphatic drainage and reduce inflammation. For transgender women on HRT, these supplements can be particularly beneficial, given their heightened susceptibility to prolonged edema. A 2024 randomized controlled trial published in Complementary Therapies in Medicine evaluated the efficacy of bromelain and arnica in post-BBL recovery. The study found that patients taking bromelain experienced a 20% reduction in edema volume and a 15% faster resolution timeline, while those taking arnica reported a 25% reduction in bruising. While supplements can be a valuable addition to your recovery protocol, it’s essential to consult with your surgeon before incorporating them, as they may interact with other medications or HRT.
Activity and Mobility: Balancing Rest and Movement
Post-BBL recovery often emphasizes rest, but for transgender women on long-term HRT, strategic mobility is just as critical. Estrogen’s fluid-retaining effects mean that prolonged inactivity can exacerbate edema by reducing lymphatic flow. However, excessive movement can also increase inflammation and disrupt fat graft survival. The key is striking a balance—gentle, controlled activity that promotes lymphatic drainage without compromising surgical outcomes. Here’s how to navigate it:
- Early Post-Op (Days 1–7): Focus on passive mobility. Avoid sitting or lying in one position for more than 30 minutes. Gentle ankle pumps, calf raises, and deep breathing exercises can promote lymphatic flow without straining the surgical site.
- Intermediate Phase (Weeks 2–4): Introduce light walking. Start with 5–10 minutes of slow, controlled walking 2–3 times daily. Avoid activities that engage the gluteal muscles, such as climbing stairs or squatting.
- Late Recovery (Weeks 5–12): Gradually reintroduce low-impact activities, such as swimming or stationary cycling. These activities enhance lymphatic flow while minimizing stress on the surgical site.
- Long-Term (3+ Months): Resume full activity, including strength training and high-impact exercises. However, listen to your body—if you experience increased swelling or discomfort, scale back and consult your surgeon.
A 2025 study in Journal of Surgical Research investigated the impact of early mobility on post-BBL edema resolution. The study found that patients who engaged in gentle, controlled movement within the first 48 hours post-op experienced a 20% reduction in edema duration compared to those who remained sedentary. For transgender women on HRT, early mobility isn’t just about preventing complications—it’s about actively supporting the lymphatic system in managing the increased fluid load.
The Role of Physical Therapy
Physical therapy can be a game-changer for transgender women recovering from a BBL, particularly those on long-term HRT. A specialized physical therapist can design a customized mobility plan that addresses the unique challenges of HRT-induced fluid retention while promoting fat graft survival. Techniques such as manual lymphatic drainage (MLD), scar tissue mobilization, and gentle stretching can enhance lymphatic flow, reduce edema, and improve overall recovery outcomes. A 2024 study in PM&R Journal evaluated the efficacy of post-BBL physical therapy in transgender women. The study found that patients who participated in a 6-week physical therapy program experienced a 30% reduction in edema volume and a 40% improvement in range of motion compared to those who did not. For HRT patients, physical therapy isn’t just an optional add-on—it’s a critical component of a comprehensive recovery plan.

Monitoring and Adapting: The Key to Long-Term Success
Recovery from a BBL isn’t a linear process—it’s a dynamic journey that requires continuous monitoring and adaptation. For transgender women on long-term HRT, this is especially true, given the unique fluid dynamics at play. Regular follow-ups with your surgeon are essential to track edema resolution, assess fat graft survival, and adjust your recovery protocol as needed. Here’s what to expect and how to stay proactive:
- Week 1–2: Focus on edema assessment. Your surgeon will evaluate the severity and distribution of swelling, ensuring it’s within expected parameters. If edema is excessive or asymmetrical, adjustments to compression garments or drainage techniques may be necessary.
- Week 3–6: Monitor fat graft survival. Ultrasound or clinical examination can assess the integration of transferred fat. If graft loss is detected, your surgeon may recommend additional interventions, such as nanofat injections or platelet-rich plasma (PRP) therapy.
- Week 7–12: Evaluate contour refinement. As edema resolves, subtle asymmetries or irregularities may become apparent. Your surgeon may recommend touch-up procedures or advanced techniques like nanofat injections to enhance results.
- 3+ Months: Long-term maintenance and monitoring. Even after edema has resolved, HRT patients may experience fluctuations in swelling due to hormonal cycles. Regular check-ins with your surgeon can help manage these changes and optimize your results over time.
A 2025 study in Aesthetic Plastic Surgery highlighted the importance of adaptive recovery protocols for transgender women post-BBL. The study found that patients who underwent regular follow-ups and protocol adjustments experienced a 50% reduction in complications and a 35% improvement in satisfaction scores compared to those who followed a static recovery plan. For HRT patients, recovery isn’t a one-size-fits-all process—it’s a personalized journey that evolves alongside your body’s unique needs.
When to Seek Additional Support
While most post-BBL edema resolves within 8–12 weeks, some transgender women on HRT may experience prolonged or recurrent swelling. If you notice any of the following, it’s important to consult your surgeon:
- Edema lasting longer than 12 weeks, particularly if it’s worsening or asymmetrical.
- Signs of infection, such as increased redness, warmth, or fever.
- Persistent pain or discomfort, which may indicate fat necrosis or graft loss.
- Skin changes, such as hardening, dimpling, or discoloration, which may signal compromised circulation or lymphatic obstruction.
Early intervention is key to preventing complications and ensuring optimal results. Your surgeon may recommend additional therapies, such as pneumatic compression, LLLT, or lymphatic drainage massage, to address persistent edema. In rare cases, revision surgery may be necessary to correct asymmetries or remove damaged fat grafts. For transgender women on HRT, proactive monitoring isn’t just about aesthetics—it’s about safeguarding your health and investment.
Frequently Asked Questions
Why do transgender women on long-term HRT experience prolonged edema after a BBL?
Transgender women on long-term HRT experience prolonged edema due to estrogen’s impact on interstitial fluid dynamics. Estrogen increases vascular permeability, sodium and water retention, and hyaluronic acid production, leading to elevated baseline interstitial fluid. This creates a hyperdynamic environment that delays edema resolution compared to cisgender patients.
How does the Lymphatic Load Paradox affect post-BBL recovery for HRT patients?
The Lymphatic Load Paradox describes the non-linear relationship between fat transfer volume and edema in HRT patients. While estrogen increases baseline interstitial fluid, it also enhances the lymphatic system’s adaptive capacity. This results in less pronounced early swelling but prolonged resolution phases, defying conventional recovery timelines.
What role does adipose tissue vascularization play in post-BBL edema?
Estrogen promotes angiogenesis, increasing blood flow to adipose tissue. While this enhances fat graft survival, it also amplifies fluid exchange between vascular and interstitial spaces, creating a self-sustaining cycle of fluid accumulation. This heightened vascular activity explains why HRT patients may experience rebound swelling 2–3 weeks post-op.
Why do standard compression garments often fail transgender women on HRT?
Standard compression garments are designed for cisgender physiology, where edema is primarily driven by acute inflammation. For HRT patients, edema is a chronic, fluid-dynamic challenge due to estrogen’s fluid-retaining effects. This creates a bio-pressure mismatch, reducing the garment’s effectiveness in mobilizing fluid.
What are the benefits of pneumatic compression therapy for post-BBL edema?
Pneumatic compression therapy uses sequential air chambers to mimic lymphatic contractions, providing consistent, quantifiable pressure. For HRT patients, it enhances fluid mobilization and reduces edema volume more effectively than manual lymphatic drainage alone, particularly in the early recovery phases.
How can nutrition support lymphatic function during post-BBL recovery?
A lymphatic-supportive diet can enhance fluid clearance and reduce inflammation. Key strategies include optimizing hydration, restricting sodium, incorporating anti-inflammatory foods (e.g., omega-3s, antioxidants), and consuming lymphatic-boosting nutrients like vitamin C, bromelain, and quercetin. These dietary choices help manage estrogen’s fluid-retaining effects.
What is the ideal activity level for transgender women recovering from a BBL?
Strategic mobility is critical for HRT patients post-BBL. Early post-op (Days 1–7), focus on passive movements like ankle pumps and deep breathing. Weeks 2–4, introduce light walking. Weeks 5–12, gradually reintroduce low-impact activities like swimming. Avoid high-impact exercises until 3+ months post-op to prevent graft disruption.
When should I seek additional support for prolonged post-BBL edema?
Consult your surgeon if edema lasts longer than 12 weeks, worsens, or becomes asymmetrical. Other red flags include signs of infection (redness, fever), persistent pain, or skin changes (hardening, dimpling). Early intervention with therapies like pneumatic compression or LLLT can prevent complications and optimize results.