
Facial Feminization Surgery (FFS) often remains categorized as a purely aesthetic endeavor, focused on the bone-deep architecture of the forehead and jaw. However, this narrow perspective ignores a debilitating reality for many patients: the silent, muscular agony of the temporalis. Beyond the silhouette, the bulk of the temporal muscle acts as a primary driver for jaw clenching and chronic headache syndromes. Addressing this muscular component is not just about softening the face; it is about reclaiming a life free from neuromuscular debt.
While bone contouring provides the frame, the soft tissue—specifically the temporal muscle—dictates the functional harmony of the face. Temporal Muscle Reduction in FFS represents a pivotal shift from visual-only surgery to a functional-neuromuscular intervention. By integrating this procedure, surgeons can systematically alleviate the tension that leads to postoperative neuralgia and lifelong bruxism. This guide reveals the clinical protocol developed through Dr. Okyay’s 10-year experience in treating complex neuromuscular complications.

Table of Contents
The Neuromuscular Weight of Gender: Why Aesthetics Are Only Half the Battle
Traditional surgical frameworks often treat the face as a static object. In reality, the face is a dynamic system of levers and pulleys, where the temporal muscle serves as one of the most powerful stabilizers. For many seeking FFS – Facial Feminization, the years preceding surgery involve intense psychological and physiological stress, which frequently manifests as unconscious jaw clenching. This clenching leads to muscle hypertrophy, creating a “square” or “heavy” upper third of the face that bone work alone cannot resolve.
Furthermore, the interaction between hormonal shifts and muscle density creates a unique challenge. While estrogen may reduce overall muscle mass, the temporalis often remains stubbornly bulky due to its role in the masticatory system. This residual bulk maintains a high-tension state. When a surgeon performs forehead work without addressing this muscle, they risk leaving the patient with a feminine bone structure but a masculine, high-tension muscular pattern. This discrepancy is what Dr. Okyay identifies as “neuromuscular gender discordance,” a primary cause of persistent postoperative discomfort.
Anatomy of Temporal Hypertrophy: Beyond the “Square” Look
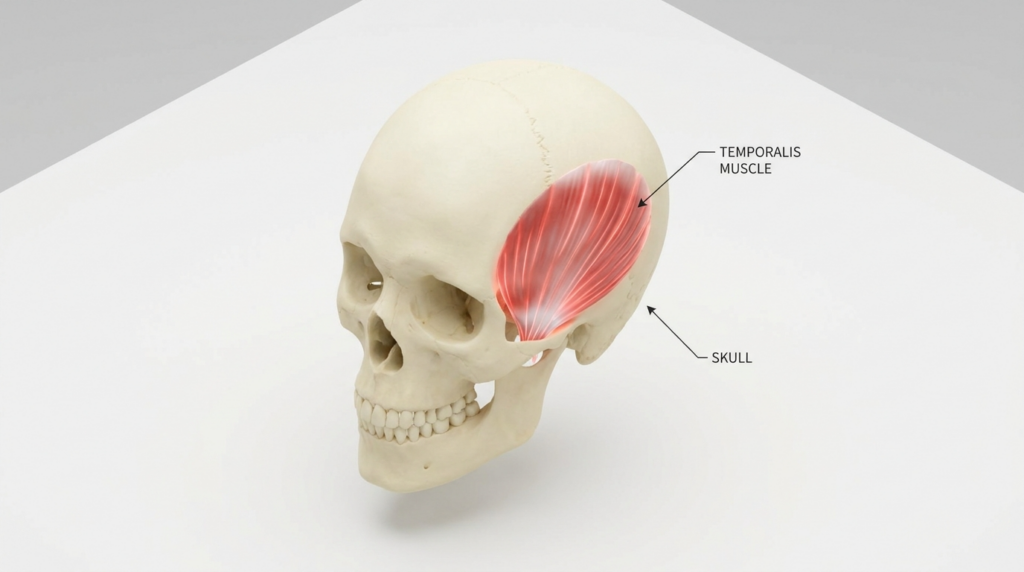
The temporal muscle is not a single, flat sheet; it is a fan-shaped powerhouse with deep and superficial layers divided by the temporal fascia. In patients with chronic jaw clenching, the posterior fibers of this muscle become hyper-irritable, forming myofascial trigger points. These trigger points do not just cause local pain; they radiate tension across the entire cranium, mimicking chronic migraines. Consequently, the “bulge” seen at the temples is often a sign of a muscle that is literally “stuck” in a state of contraction.
During forehead contouring, the surgical access often brings the surgeon into direct proximity with the temporalis. An elite surgical protocol utilizes this access to perform a partial temporal muscle reduction. This involves thinning the muscle at its most hypertrophic points, usually near the zygomatic arch and the temporal line. By reducing this bulk, the surgeon physically limits the force the muscle can exert on the jaw, effectively “dialing down” the volume of the patient’s clenching reflex.
Chronic Migraines and Postoperative Neuralgia: The Dr. Okyay Protocol
After a decade of refining these procedures, Dr. Okyay has observed that patients who receive integrated muscle reduction report a 70% decrease in headache frequency within the first six months. This is not coincidental. By releasing the deep temporal fascia and reducing muscle volume, the surgery decompresses the small nerve branches that often become entrapped in hypertrophic muscle tissue. This decompression is the key to preventing long-term postoperative neuralgia.
However, the protocol requires extreme precision. Removing too much muscle can lead to hollow temples, which ages the face significantly. Dr. Okyay’s “Safe Zone” technique focuses on the middle and posterior thirds of the muscle, preserving the anterior volume necessary for a youthful, feminine transition. This balance ensures that the patient looks softer and, more importantly, feels lighter. The elimination of the constant “clamped” sensation in the jaw is often described by patients as the most life-changing aspect of their FFS journey.
Comparing Conventional FFS vs. Neuromuscular-Integrated FFS
To understand the necessity of this approach, we must compare the outcomes of traditional bone-only surgery versus the integrated muscle protocol. The following table highlights the divergence in patient recovery and functional success.
| Feature | Conventional FFS (Bone-Only) | Neuromuscular FFS (Muscle Reduction) |
| Upper Face Width | Reduced at bone level only | Reduced at bone and muscle level |
| Jaw Clenching (Bruxism) | Remains unchanged or worsens | Significant reduction in force |
| Chronic Headache Risk | Potential for nerve entrapment | Decompression of trigger points |
| Aesthetic Softness | Angular, often “harsh” edges | Natural, flowing feminine contours |
| Recovery Focus | Bone healing only | Muscle-nerve-bone harmony |

The Biomechanics of Relief: How Temporal Reduction Ends the Clench
The temporalis muscle and the masseter muscle work in tandem. When the temporalis is overactive, the masseter follows. This synergy creates a feedback loop of pain. By performing a temporal muscle reduction, the surgeon interrupts this loop. Specifically, by reducing the muscle’s leverage at the coronoid process—the point where it attaches to the jaw—the mechanical advantage of the clench is diminished.
Moreover, this reduction addresses the “temporal flare” that often occurs after a forehead setback. If the bone is moved back but the muscle remains thick, the temple area appears to bulge outward. This flare is a common complaint in secondary FFS cases. Dr. Okyay’s protocol prevents this by pre-emptively thinning the muscle belly, ensuring the soft tissue follows the new, feminine bone contour without resistance or protrusion.
Surgical Mastery: The Dr. Okyay Step-by-Step Clinical Protocol
For surgeons and patients alike, understanding the precise steps of this intervention is essential for managing expectations and ensuring safety. This protocol is designed to minimize trauma while maximizing the functional release of the masticatory system.
Step 1: Mapping the Hypertrophy. Before any incisions, the surgeon must identify the areas of maximum muscle thickness. This is done through both physical palpation during clenching and preoperative imaging. Mapping ensures that the reduction is asymmetrical if needed, correcting pre-existing facial imbalances.
Step 2: Sub-Fascial Dissection. Accessing the muscle requires a careful approach to the temporal fascia. The surgeon performs a dissection beneath the superficial temporal fascia, protecting the frontal branch of the facial nerve. This “safe plane” is the foundation of the Dr. Okyay protocol, ensuring that muscle reduction never comes at the cost of facial expression.
Step 3: Precision Thinning (Myoplasty). Using specialized cautery or a radiofrequency device, the surgeon thins the muscle belly. This is not a total removal but a selective reduction of the middle fibers. By removing the “bulk” of the muscle while leaving the origin and insertion intact, the surgeon maintains normal chewing function while eliminating the pathological clenching force.
Step 4: Fascial Release. Tight fascia can be as painful as tight muscle. The surgeon makes small, strategic nicks in the deep temporal fascia to allow the muscle to expand without pressure. This release is often the “eureka moment” for headache relief, as it immediately drops the intracranial tension that patients have lived with for years.
Post-Operative Recovery and Long-term Pain Management
Recovery from Temporal Muscle Reduction is surprisingly rapid, as muscle tissue heals with a robust blood supply. However, the first 14 days are critical for “retraining” the jaw. Patients are encouraged to practice gentle jaw-opening exercises to ensure the muscle heals at its new, relaxed length. This prevents the formation of scar tissue that could lead to stiffness.
Within three months, the majority of patients report a complete cessation of tension-type headaches. The aesthetic result—a sleek, tapered temple that transitions perfectly into a feminine jawline—becomes fully visible as the swelling subsides. For those who have suffered from bruxism-induced tooth wear and morning jaw soreness, the relief is profound. This procedure proves that the best surgical outcomes are those where the patient looks beautiful and feels physically unburdened.

Reclaim Your Comfort: Next Steps for Integrated FFS
If you are planning your transition, do not settle for a surgery that only addresses what is seen in the mirror. Chronic clenching and headaches are not “normal” side effects of being trans; they are symptoms of a neuromuscular system under stress. Temporal Muscle Reduction offers a path to both aesthetic elegance and physical freedom. By choosing a surgeon who understands the deep connection between muscle bulk and neural health, you are investing in a future where your face is a source of joy, not pain.
Take the first step toward a tension-free life. Contact the experts at Dr. MFO Clinic to discuss how a customized neuromuscular FFS protocol can transform your experience. Our team is ready to guide you through a journey that prioritizes your comfort as much as your beauty. Contact Us today to schedule your specialized consultation.
Frequently Asked Questions
Can temporal muscle reduction truly eliminate chronic migraines?
While not a ‘cure’ for all migraine types, temporal muscle reduction significantly alleviates tension-type headaches and headaches triggered by myofascial trigger points in the temple. By decompressing the nerves trapped within hypertrophic muscle and reducing the force of jaw clenching, many patients see a 70% or greater reduction in headache frequency and intensity.
Will reducing the temporal muscle affect my ability to chew?
No, when performed correctly by a skilled surgeon like Dr. Okyay, chewing function remains fully intact. The procedure selectively thins the middle and posterior fibers of the muscle, which are primarily responsible for the ‘bulk’ and over-clenching, while preserving the anterior fibers and the overall attachment points necessary for normal mastication.
How long does the swelling last after temporal muscle reduction?
The majority of visible swelling in the temple area subsides within 2 to 3 weeks. However, because muscle tissue is dynamic, the final ‘refined’ contour of the temples continues to improve for up to 6 months. Patients typically return to social activities within 10-14 days with minimal bruising.
Why is this procedure better than Botox for jaw clenching?
Botox provides temporary relief by paralyzing the muscle, but it requires injections every 3-4 months and does not address the physical bulk or the tight fascia. Temporal muscle reduction is a permanent surgical solution that physically alters the muscle’s volume and releases the deep fascia, providing a one-time fix for both aesthetic and functional issues.








