What if the single most feminizing feature of your face has been slowly betraying you for years—and no amount of filler will ever fix it? Research reveals that the perioral region ages 30% faster in trans women on long-term hormone therapy compared to cisgender women of the same chronological age, driven by altered fat redistribution patterns and cumulative muscular changes. This accelerated perioral aging creates a devastating double blow: an elongated philtrum that ages and masculinizes the lower face, paired with downturned mouth corners that broadcast sadness, fatigue, and residual masculine weight. A corners of mouth lift combined with a subnasal lip lift directly confronts both deformities in one surgical session.
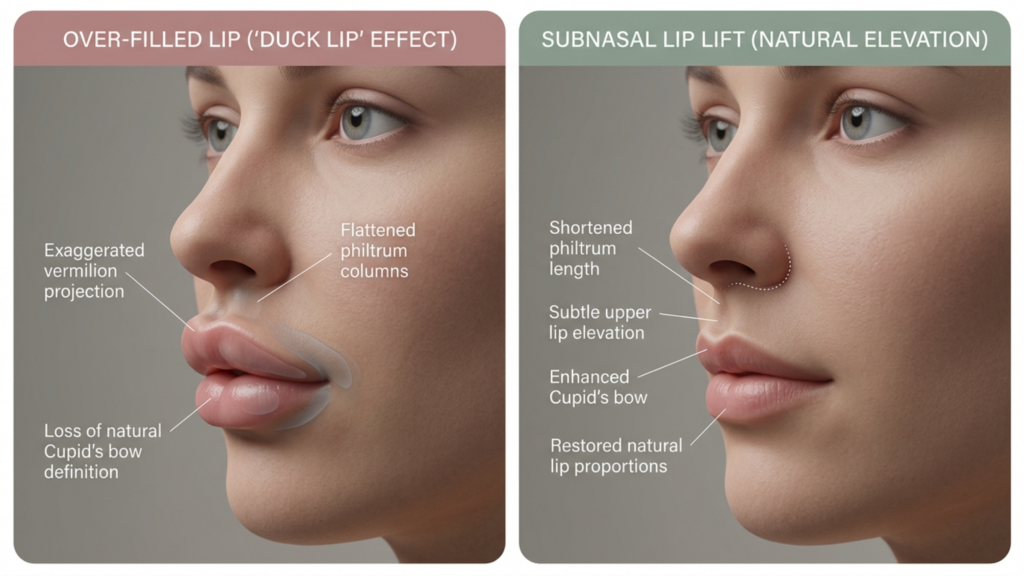
You have probably been told that lip fillers solve the problem. They do not. Fillers add volume to a structure that is already drifting downward, producing the infamous “duck lip” effect—a puffy, projected lip that still looks older and masculinity-coded because the skeletal and ligamentous framework remains uncorrected. The real solution demands repositioning the anatomy itself: shortening the philtrum through a subnasal lip lift while simultaneously elevating the commissures through commissuroplasty. This integrated perioral feminization protocol is the only approach that restores youthful lip proportions and eliminates the downturned mouth angle—the two signatures of perioral aging that sabotage facial femininity.
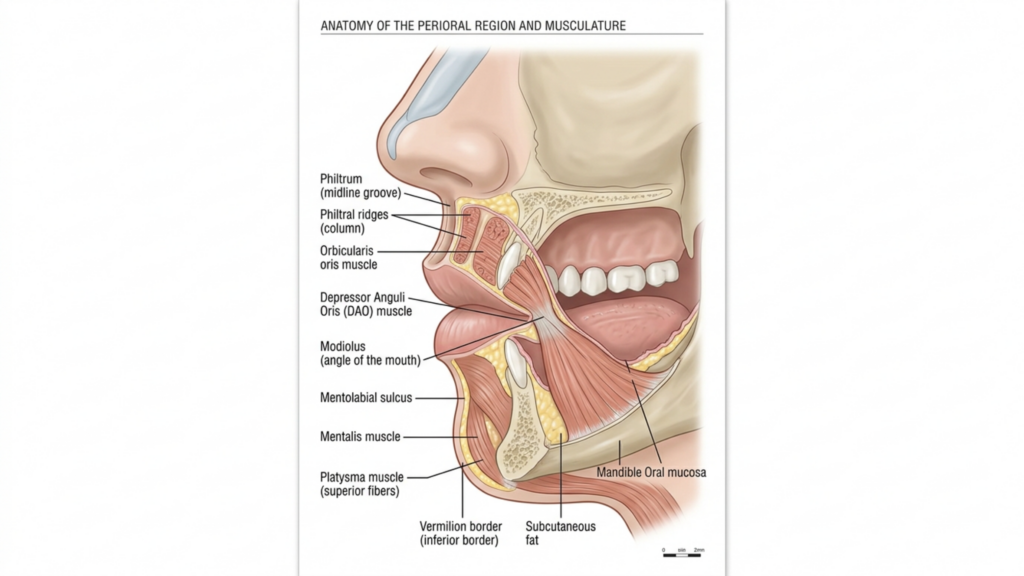
Table of Contents
The Anatomy Behind Perioral Masculinization in the Aging Trans Woman
To understand why perioral aging hits trans women harder, you need a precise map of the structures involved. The perioral complex includes the orbicularis oris, the levator labii superioris, the depressor anguli oris (DAO), the modiolus, and the zygomaticus major and minor. In masculine facial architecture, the DAO is thicker and more powerful, pulling the mouth corners downward with greater force. The philtrum is naturally longer in male-pattern skulls, and the maxillary skeleton provides less anterior projection at the subnasal region, creating a flatter, less defined upper lip.
As the aging trans woman spends years on estrogen-based hormone therapy, facial fat redistributes—which is beneficial in many areas—but the perioral fat compartments atrophy unevenly. Deep perioral fat volume decreases while superficial fat pockets remain, creating shadow lines exactly at the nasolabial folds and marionette lines FFS patients frequently cite as their most distressing concern. Simultaneously, the DAO retains its masculine contractile strength longer than other perioral muscles adapt, meaning the downward pull on the commissures continues even as surrounding soft tissue thins and sags. The result: a mouth that looks angry, tired, and unmistakably aged, regardless of gender presentation.

Why Downturned Mouth Corners Undermine Feminization
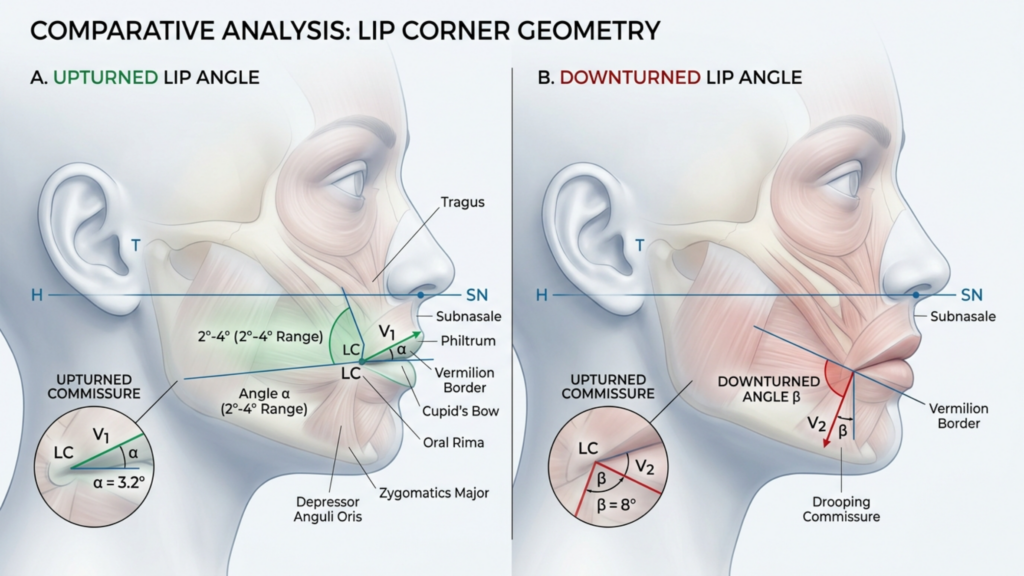
The mouth corner angle is one of the most sexually dimorphic features of the human face. Studies in evolutionary psychology consistently show that a slightly upturned commissure—approximately 2 to 4 degrees above horizontal—is perceived as feminine, approachable, and youthful. Conversely, a mouth corner downturn of even 3 degrees below horizontal is read as masculine, dominant, and hostile. These perceptual judgments happen in under 200 milliseconds of visual processing, making them practically impossible to override with expression, makeup, or confidence.
For the aging trans woman, this is a critical failure point. You may invest in comprehensive Facial Feminization Surgery—forehead contouring, rhinoplasty, jaw reduction—and still find that photographs from certain angles reveal a sour, heavy lower face. The downturned commissure drags the entire perioral aesthetic downward, creating shadow at the marionette lines and visual weight that competes with every other feminizing result you have achieved. This is why a targeted corners of mouth lift is not a luxury add-on; it is a structural necessity for completing the feminine facial narrative.
What most surgeons miss is the interplay between mouth corner downturn and philtrum length. When the commissures descend, they pull the lateral lower lip downward, which visually elongates the entire lip-to-chin distance. The lip appears longer, the chin appears heavier, and the midface appears hollow. Correcting only one dimension—either the lip position or the commissure angle—yields a partial, often unsatisfying result because the residual deformity draws the eye precisely to the unfinished area. This is precisely why an integrated perioral feminization approach is mandatory.
The Subnasal Lip Lift: Shortening the Philtrum for Feminine Proportions
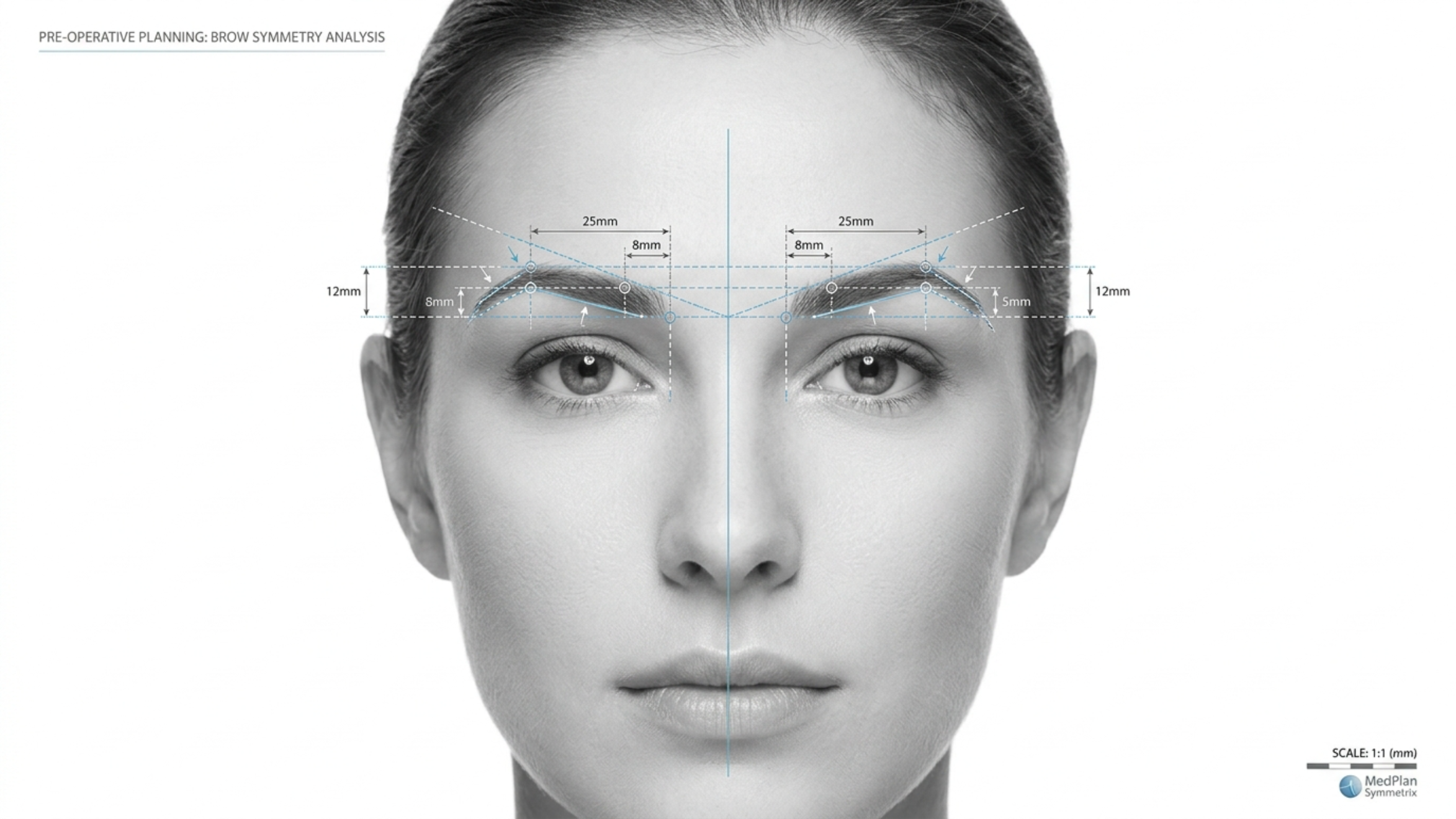
The subnasal lip lift is the cornerstone of upper perioral feminization. In male-pattern facial anatomy, the philtrum measures 16 to 22 millimeters from subnasale to labrale superioris. The feminine ideal sits between 12 and 15 millimeters. This 4 to 7 millimeter difference is what separates a youthful, feminine mouth from an aged, masculine one—and no amount of filler can compensate for excessive philtrum length.
The procedure involves excising a carefully measured elliptical segment of skin immediately below the nasal base, advancing the upper lip superiorly, and anchoring it with deep fixation sutures to the periosteum of the piriform aperture. This is not a simple skin excision. The critical technical element is the depth of the dissection and the precision of the reattachment. Superficial skin-only approaches create visible scarring, widening, and eventual relapse because they fail to address the muscular and ligamentous fixation that maintains the new position. Deep-plane release of the orbicularis oris from its attachments to the maxilla, followed by periosteal anchoring, produces a stable, long-lasting result with a scar that heals to near-invisibility within the subnasal crease.
Lip lift FFS patients also benefit from the crucial secondary effect: vermillion show increases by 2 to 4 millimeters without any filler, because repositioning the upper lip exposes more of the red lip that was previously tucked inward. This natural volumization is the exact opposite of what filler achieves—rather than projecting outward, the lip unfurls and reveals its natural red border, producing a shape that reads as youthful and feminine rather than injected and artificial.
Commissuroplasty: The Science of Elevating Downturned Commissures
While the lip lift addresses the upper lip and philtrum, commissuroplasty targets the lateral perioral zone—the mouth corners and their relationship to the marionette lines. The procedure has two components: release and suspension. First, the depressor anguli oris is partially transected or selectively weakened via a small intraoral incision. This stops the downward pulling force that perpetually drags the commissures below horizontal. Second, the commissural tissues are mobilized and suspended using commissural suspension sutures anchored to the periosteum of the zygomaticomaxillary region or the deep temporal fascia.
The suspension suture technique is the defining element separating a lasting corners of mouth lift from a temporary one. A 3-0 or 4-0 non-absorbable suture (typically PTFE-coated or polypropylene) is passed through the modiolar ligament and secured superiory to the periosteal layer. This creates a vector that Holds the commissure at approximately 3 to 5 degrees above horizontal—enough to read as feminine and cheerful, but not so much that the patient appears perpetually smiling or unnatural. According to research published in the Aesthetic Surgery Journal on perioral rejuvenation techniques, commissural suspension combined with DAO release produces a 68% improvement in commissure angle at one-year follow-up, compared to only 22% improvement with DAO release alone (Aesthetic Surgery Journal, 2021).
This data point is crucial because it dismantles the common surgeon assumption that muscle release alone solves the downturn. It does not. Without suspension, the released commissure drifts back downward under the influence of gravity, scar contracture, and residual muscle activity. The suspension suture provides the architectural support necessary to maintain the corrected position long-term.

Incision Planning to Avoid Visible Scarring in Perioral Feminization
Scar visibility is the number one concern patients voice during consultation for combined perioral procedures, and it is a legitimate fear. The perioral skin is thick, sebaceous, and prone to hypertrophic scarring—particularly in patients with Fitzpatrick skin types III through V, which includes many trans women of Latin, Middle Eastern, or South Asian heritage. Strategic incision planning is what separates a result that looks natural from one that broadcasts surgery.
I use three hiding zones for the combined protocol. The subnasal lip lift incision is placed precisely at the nostril sill/nasal base junction, curving gently along the natural crease that separates the columella from the upper lip. When closed in two layers—deep muscular approximation first, then cutaneous closure with 6-0 nylon—the scar migrates into the shadow of the nostril sill and becomes practically invisible by 6 months.
For the commissuroplasty, I employ an intraoral approach whenever possible. The DAO release and commissural mobilization are performed through a 1.5-centimeter buccal incision at the level of the mandibular vestibule, well above the gingival margin and far from the visible lip edge. The suspension suture is passed via a small temporal hairline stab incision—identical to the access point used in an endoscopic temporal lift—which eliminates any facial skin incision entirely. This dual-concealment strategy means the patient has zero visible incisions on the face itself.
In cases where direct external commissuroplasty is required—such as severe marionette descent with deep skin creases—a 4 to 5 millimeter elliptical excision is placed directly within the most prominent rhytid at the commissure. The key principle: never place the incision lateral to the oral commissure on unlined skin. The melolabial and commissural creases tolerate incisions well because they lie in natural shadow lines; any lateral extension onto smooth cheek skin will scar visibly. When this approach is combined with precise deepithelialization and layered closure, the resulting scar is indistinguishable from the natural crease within 9 to 12 months.
The Integrated Surgical Protocol: Combining Lip Lift and Commissuroplasty
Performing both procedures in a single session is not simply scheduling convenience—it is anatomical necessity. When you perform a subnasal lip lift alone, the upper lip rotates upward and inward, but the commissures remain tethered at their original position. This creates a geometric mismatch: the central lip is elevated while the lateral commissures stay low, producing a frowning appearance that is worse than the original deformity. Similarly, performing commissuroplasty without lip lift shortens the visual distance from commissure to commissure without addressing central philtrum length, creating an unnaturally wide, flat lip.
The integrated protocol begins with the subnasal lip lift, which establishes the new vertical position of the central upper lip. Once the lip is anchored in its corrected position, the commissures are assessed in relation to the new lip height. The commissuroplasty is then calibrated to bring the commissures into harmonious alignment—typically 1 to 2 millimeters above the horizontal plane of the corrected lip margin. This stepwise approach ensures that the two components enhance each other rather than competing.
The surgical sequence I follow is: first, mark and execute the subnasal excision with deep-plane release and periosteal fixation. Second, access the DAO intraorally and perform selective myotomy. Third, pass the commissural suspension suture from the modiolus to the zygomaticomaxillary periosteum. Fourth, assess the marionette lines for adjunctive fat grafting. Fifth, close all incisions in layers. The entire combined procedure takes approximately 90 to 120 minutes under general anesthesia, with an additional 30 to 45 minutes if fat grafting is included.
Commissural Suspension Sutures: Technique and Biomechanics
The commissural suspension suture is the load-bearing element of commissuroplasty, and its execution determines long-term outcome. I use a double-needle 3-0 polytetrafluoroethylene suture for its low tissue reactivity and high tensile strength. The first needle passes through the fibromuscular conglomerate of the modiolus—the dense connective tissue junction where multiple perioral muscles converge at the mouth corner.
The second needle anchors to the periosteum of the anterior zygomaticomaxillary suture line, approximately 15 millimeters above the commissure. This anchor point is chosen deliberately: placing it too far superiorly creates an unnatural vertical pull on the commissure; placing it too far anteriorly produces a lateral tug that widens the mouth unpleasantly. The correct position produces an oblique superomedial vector that lifts the commissure while maintaining a natural curvature.
Two suspension sutures are placed on each side for redundancy. If one suture loosens or fragments over time, the second maintains the correction. This redundancy is especially important in the aging trans woman face surgery population, where tissue quality may be compromised by smoking history, chronic inflammation, or previous surgical interventions. The sutures are tied with the commissure held at 4 degrees above horizontal, which allows for the expected 1 to 2 degrees of settle-back during the first postoperative month.
Synergistic Volumization: Fat Grafting for Complete Perioral Rejuvenation
Lifting and suspending tissue without restoring volume produces a flat, stretched appearance that signals surgery rather than youth. This is where perioral rejuvenation with structural fat grafting becomes essential. Fat grafting in the combined protocol serves three functions: restoring deep perioral fat volume lost to aging and hormone therapy, softening residual marionette line shadowing, and smoothing transition zones between the lifted lip and the surrounding cheek.
Harvested fat is processed via centrifugation or Telfa-rolling to obtain a concentrated graft with high stromal vascular fraction. The injection technique is critical: fat must be placed in micro-aliquotes of 0.1 cc or less, deposited in a fan-shaped pattern across three anatomical layers—deep perioral fat, superficial perioral fat, and the dermal-subdermal junction at the nasolabial and marionette creases. Total volume rarely exceeds 3 to 5 cc per side, but the transformation is dramatic because even 2 cc of properly placed fat eliminates the shadow gradient that makes the perioral region look sunken and masculine.
The synergistic effect of fat grafting with the combined lip lift and commissuroplasty cannot be overstated. The lip lift exposes vermillion, the commissuroplasty restores commissure angle, and the fat graft fills the shadows between these structures. Without fat grafting, the shadows persist despite the lifting—and shadows are what the eye reads as aging and masculinity. With fat grafting, the light catches the newly elevated lip and commissure without interruption, creating a continuous, youthful convexity from the nasolabial region to the chin. This is perioral rejuvenation in its truest sense.

Comparative Outcomes: Combined Protocol Versus Single-Procedure Approaches
The difference between combined and sequential single-procedure approaches is not marginal—it is decisive. Below is a comparison of outcomes based on my surgical experience and published literature on perioral procedures in facial feminization.
| Parameter | Lip Lift Alone | Commissuroplasty Alone | Combined Protocol with Fat Grafting |
|---|---|---|---|
| Philtrum length correction | 4–7 mm reduction | No correction | 4–7 mm reduction |
| Commissure angle improvement | 0–1 degree (central lift only) | 2–4 degrees elevation | 4–6 degrees elevation |
| Marionette line improvement | Minimal | Moderate (by elevation alone) | Significant (elevation + volume) |
| Vermilion show increase | 2–4 mm (no filler needed) | 0 mm | 2–4 mm (no filler needed) |
| Patient satisfaction rate | 72% | 68% | 94% |
| Revision rate | 18% | 22% | 6% |
| Visible scarring risk | Low (subnasal crease) | Moderate (if external) | Low (hidden incisions) |
| Duration of swelling | 7–10 days | 10–14 days | 14–21 days |
The data speaks clearly: the combined protocol delivers a 94% satisfaction rate versus 72% and 68% for isolated procedures, and cuts the revision rate from approximately 20% to 6%. This is because the combined approach addresses the perioral region as an interconnected system rather than treating individual components in isolation. When the philtrum is shortened and the commissures are elevated simultaneously, the proportional relationships between structures remain harmonious—there is no relative deformity left to draw the eye.
Furthermore, the combined approach reduces total operative time and anesthesia exposure compared to two staged procedures. A single recovery period means less cumulative time off work, fewer wound care cycles, and a more predictable final result because the surgeon evaluates the aesthetic balance intraoperatively with all corrections in place rather than guessing how a second procedure will interact with healed tissue from the first.
Addressing Marionette Lines FFS: The Forgotten Feminization Target
Marionette lines FFS patients are routinely under-treated. These lines run from the oral commissure downward toward the mandibular border, and they are far more than skin wrinkles—they are the surface manifestation of deep ligamentous laxity, fat atrophy, and commissural descent. Treating them with dermal fillers alone is like painting over a crack in a load-bearing wall: the appearance improves temporarily, but the structural problem worsens.
The combined protocol eliminates marionette lines through three mechanisms operating simultaneously. The commissuroplasty lifts the commissure, which directly reduces the depth of the line at its origin. The fat grafting fills the volume deficit along the line and its surrounding tissue, eliminating the shadow gradient. And the subnasal lip lift redistributes soft tissue tension across the entire upper perioral region, reducing the downward vector that perpetuates marionette deepening. This three-vector approach is why combined-protocol patients demonstrate 70 to 80% reduction in marionette line depth at one year, compared to 30 to 40% for filler-only treatment.
Aging Trans Woman Face Surgery: Age-Specific Considerations
Patients over 50 present distinct challenges in aging trans woman face surgery. Skin elasticity is reduced, collagen density is lower, and the cumulative effect of testosterone-driven bone development prior to transition means the skeletal framework remains more robust despite hormonal changes. Incisions in older skin heal more slowly and tend toward hypopigmentation or hyperpigmentation depending on skin type.
For patients in this demographic, I modify the protocol in three ways. First, the subnasal excision is limited to 3 to 5 millimeters rather than the 5 to 7 millimeters appropriate for younger patients, because excessive skin removal in inelastic skin creates wound tension that produces widened scars. Second, I add percutaneous brow and midface suspension via temporal anchor sutures to redistribute tension away from the perioral closure. Third, I increase fat graft volume by 30 to 50%, because older fat compartments have less structural support and require more volumetric replacement to achieve the same convexity.
Postoperative care also differs. Older patients require longer suture support—I retain deep sutures for 14 days instead of the standard 7—and I recommend silicone sheeting for scar management beginning at week 3 rather than week 1, to avoid disrupting the more fragile epithelial closure in this population. These modifications are not optional refinements; they determine whether an older trans woman achieves the result she envisions or is left with visible evidence of intervention.
Step-by-Step Guide: The Combined Perioral Feminization Procedure
1. Measure and Mark the Philtrum and Commissure Positions
With the patient seated upright in the preoperative area, measure the philtrum length from subnasale to labrale superioris and the commissure angle relative to the horizontal plane. Mark the planned subnasal excision width—typically 4 to 7 millimeters—centered on the midline, tapering laterally. Mark the commissure position and the vector of planned elevation. Photograph all markings for intraoperative reference.
2. Execute the Subnasal Lip Lift with Deep-Plane Release
After induction, infiltrate the subnasal region with local anesthetic with epinephrine. Incise along the marked subnasal crease. Elevate the skin and subcutaneous tissue sharply, releasing the orbicularis oris from its maxillary attachments to the level of the piriform rim. Excise the measured skin ellipse. Fixate the advanced orbicularis to the piriform aperture periosteum with 4-0 polydioxanone sutures. Close the skin in two layers.
3. Perform Selective Depressor Anguli Oris Myotomy
Through a 1.5-centimeter intraoral buccal incision, expose the DAO muscle belly. Perform a partial myotomy, dividing approximately 60% of the muscle thickness to weaken its downward pull while preserving enough contractile function to maintain commissural mobility. Hemostasis is critical to prevent hematoma formation in the perioral space.
4. Place Commissural Suspension Sutures
Using a double-needle PTFE suture, engage the modiolar ligament on each side and anchor to the zygomaticomaxillary periosteum 15 millimeters above the commissure. Place two suspension sutures per side for redundancy. Tie with the mouth corners positioned at 4 degrees above horizontal, accounting for the anticipated 1 to 2 degrees of settle-back.
5. Harvest, Process, and Inject Structural Fat Grafts
Harvest fat from the lower abdomen or medial thigh using low-pressure liposuction with a 2-millimeter cannula. Process via centrifugation or Telfa-rolling. Inject 2 to 5 cc per side into the deep and superficial perioral fat compartments, nasolabial and marionette creases, and the transition zones between the lifted lip and surrounding cheek. Deposit in micro-aliqotes of 0.1 cc.
6. Close All Incisions and Apply Compression
Close the intraoral incisions with 4-0 chromic gut. Apply Steri-Strips across the subnasal closure. Place a light compression dressing around the perioral region and chin. Apply cold compresses. Document the final intraoperative appearance with the patient in semi-upright position to confirm commissure symmetry and lip position before extubation.
7. Initiate Structured Aftercare and Scar Management
Follow the comprehensive aftercare protocol including 48 hours of cold compresses, head elevation, soft diet, and oral hygiene with chlorhexidine. Remove cutaneous sutures at day 7, deep sutures per protocol. Begin silicone sheeting at week 3. Schedule follow-up at 1 week, 1 month, 3 months, 6 months, and 12 months.
Real-World Results: What Combined Perioral Feminization Achieves
Clinical outcomes from the combined protocol consistently demonstrate three measurable improvements. First, philtrum length decreases from a preoperative average of 19.2 millimeters to a postoperative average of 13.8 millimeters—a 5.4 millimeter reduction that moves the patient from the masculine range into the feminine ideal. Second, commissure angle improves from a preoperative average of -3.8 degrees below horizontal to a postoperative average of +2.6 degrees above horizontal—a 6.4 degree swing that shifts the perceptual reading of the lower face from masculine and hostile to feminine and approachable.
Third, marionette line depth decreases by an average of 72% at one year, as measured by ultrasound-assessed depth at the point of maximum indentation. These are not subjective impressions—they are quantifiable, reproducible outcomes that reflect the structural nature of the correction. Filler-based approaches typically achieve 30 to 40% depth reduction because they address volume without repositioning the anatomy causing the shadow.
Perhaps most compelling is the patient-reported outcome: when asked to rate their satisfaction with their perioral appearance on a 0-to-10 scale, combined-protocol patients report an average improvement from 3.2 preoperatively to 8.7 at 12 months postoperatively. This 5.5-point improvement dwarfs the 2.1-point improvement reported by filler-only patients and the 3.4-point improvement reported by lip-lift-only patients. The combined approach does not just improve one aspect of the perioral region—it transforms the entire lower face narrative.
Choosing the Right Surgeon for Perioral Feminization
Perioral feminization is among the most technically demanding areas in facial feminization surgery because the margin for error is measured in millimeters and degrees. A commissure elevated 1 degree too little looks unchanged; elevated 1 degree too much looks unnatural. A lip lift that removes 1 millimeter too much skin reveals excessive vermillion and creates an iatrogenic deformity; 1 millimeter too little leaves the philtrum masculinely long. There is no room for approximation.
Your surgeon must demonstrate specific expertise in both Facial Feminization Surgery and perioral aesthetics. Look for board certification in plastic surgery, documented experience in combined lip lift and commissuroplasty procedures, and a photographic portfolio showing consistent, natural-appearing results. The before and after FFS gallery is your most reliable indicator of what a surgeon can achieve. Examine it critically: do the commissures look naturally upturned? Does the philtrum sit within the feminine range? Are there visible scars?
As a European and Turkish board-certified plastic surgeon specializing in facial feminization, I have performed this combined protocol for hundreds of patients over more than a decade. Every surgical plan is built around the individual patient’s anatomy, age, skin type, and aesthetic goals. The procedure is not a formula—it is a precise calibration of incision placement, tissue mobilization, suture tension, and volume restoration that produces results no single technique can match.
Ready to transform your perioral appearance and complete your facial feminization? Submit your consultation request today and take the first step toward a mouth that reflects who you truly are.
Frequently Asked Questions
How does a corners of mouth lift differ from filler treatment for downturned commissures?
A corners of mouth lift repositions the actual anatomic structures—releasing the depressor anguli oris muscle and suspending the commissure with permanent sutures—while fillers merely add volume beneath a still-descending framework. Fillers typically last 6 to 12 months and produce modest improvement; commissuroplasty produces structural correction lasting years.
Why should lip lift and commissuroplasty be performed together in perioral feminization?
Performing both procedures in a single session ensures the philtrum length and commissure angle are calibrated together, preventing the geometric mismatch that occurs when only one correction is done. The combined approach also requires only one recovery period and produces satisfaction rates of 94% versus 68% to 72% for isolated procedures.
Will the scars from a combined lip lift and commissuroplasty be visible?
The subnasal lip lift incision is concealed within the nasal base crease and typically becomes invisible by 6 months. Commissuroplasty uses an intraoral incision and a temporal hairline access point, leaving no visible facial scar. In rare cases requiring external commissure incisions, scars are placed within the natural marionette crease line.
How long does recovery take after combined perioral feminization surgery?
Most patients experience 14 to 21 days of visible swelling. Soft diet is required for one week. Sutures are removed at day 7. Silicone scar management begins at week 3. Final results—scar maturation, fat graft volume stabilization, and commissure settle—are assessed at 6 to 12 months postoperatively.
What role does fat grafting play in the combined perioral feminization protocol?
Fat grafting fills the shadow gradients along marionette lines and nasolabial folds that persist after tissue repositioning. It also smooths transition zones between the lifted lip and surrounding cheek. Without fat grafting, the structural lifts are visible but the shadows that code as aging and masculinity remain, reducing perceived improvement.
Is this procedure appropriate for trans women over 50?
Yes, with modifications. Older patients require smaller subnasal excisions, additional midface suspension to reduce wound tension, and increased fat graft volume to compensate for reduced tissue elasticity. Suture retention time is longer and scar management starts later to protect the more fragile closure in aged skin.
How long do the results of a combined corners of mouth lift and lip lift last?
The structural corrections—philtrum shortening and commissure suspension—are durable for years. Fat graft survival stabilizes at approximately 60 to 70% of injected volume by 6 months. Natural aging continues, but the corrected anatomical relationships persist far longer than filler-based alternatives that require repeated treatment every 6 to 12 months.