
In the high-stakes world of cranioplasty, where millimeter-level precision separates success from complications, surgeons rely on advanced MRI sequences to navigate the complexities of the cranial anatomy. Among these, T1-weighted and FLAIR (Fluid-Attenuated Inversion Recovery) sequences stand out as indispensable tools. But why? The answer lies in their unique abilities to reveal critical details about the frontal bone, cerebrospinal fluid (CSF), and brain tissue—details that can make or break surgical outcomes. This article dives deep into the radiological mechanics behind these sequences, their clinical applications in cranioplasty planning, and how surgeons interpret their findings to ensure both structural integrity and functional recovery.
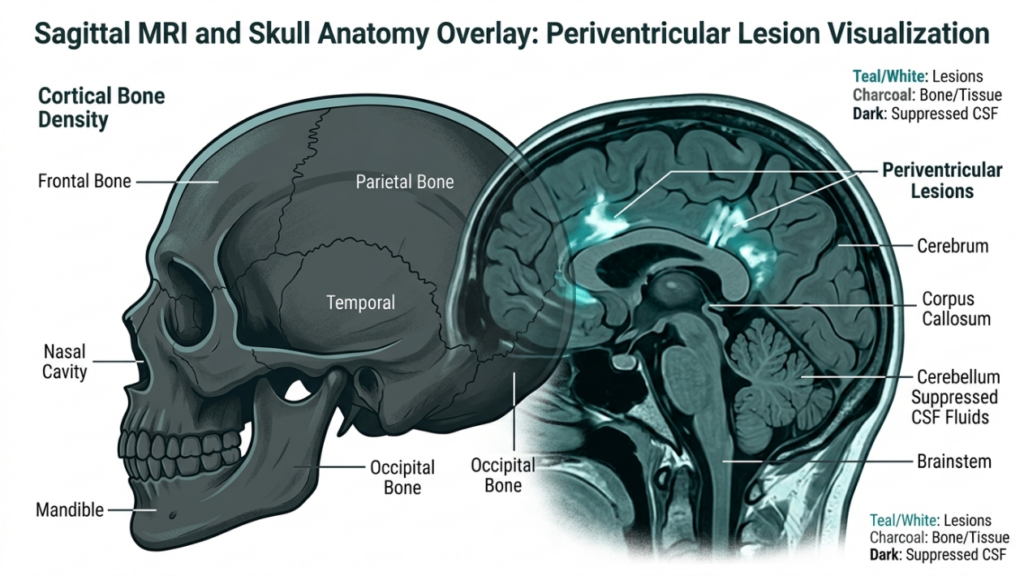
Table of Contents
The Role of T1-Weighted MRI in Cranioplasty Planning
T1-weighted MRI is the gold standard for visualizing anatomical structures with high contrast. In the context of cranioplasty, it excels at delineating the cortical bone of the skull, which appears hypointense (dark) due to its low proton density and rapid T1 relaxation time. This contrast allows surgeons to:
- Assess Bone Integrity: T1-weighted images reveal fractures, defects, or areas of demineralization in the frontal bone, which are critical for determining the feasibility of autologous bone grafts or synthetic implants. Studies have shown that T1 sequences can detect subtle cortical bone abnormalities that may be missed on CT scans, particularly in patients with complex trauma histories (Black Bone MRI, 2025).
- Evaluate Soft Tissue Interfaces: The interface between the dura mater and the frontal bone is clearly visible on T1-weighted images, helping surgeons plan the surgical dissection path to avoid inadvertent dural tears or CSF leaks.
- Identify Fat and Hemorrhage: Fat-containing structures (e.g., bone marrow) appear hyperintense (bright) on T1-weighted images, while acute hemorrhage may present as a hypointense signal. This differentiation is vital for assessing post-traumatic changes or infection risks.
However, T1-weighted MRI is not without limitations. Its inability to suppress CSF signal means that periventricular lesions or areas of edema near the frontal lobes may be obscured by the high signal intensity of CSF. This is where FLAIR sequences become indispensable.
FLAIR MRI: Suppressing CSF to Unmask Pathology
FLAIR (Fluid-Attenuated Inversion Recovery) sequences are designed to nullify the signal from CSF, making them ideal for detecting subtle abnormalities in brain tissue that might otherwise be hidden. In cranioplasty planning, FLAIR sequences are particularly valuable for:
- Detecting Periventricular Lesions: FLAIR sequences suppress the CSF signal, allowing surgeons to identify hyperintense lesions near the ventricles—common in patients with a history of trauma, infection, or demyelinating diseases. This is critical for avoiding areas of potential postoperative complications such as seizures or CSF leaks (FLAIR MRI Guide, 2026).
- Assessing Brain Parenchyma: By suppressing CSF, FLAIR enhances the visibility of cortical and subcortical abnormalities, such as gliosis or encephalomalacia, which may influence the choice of cranioplasty material or surgical approach.
- Evaluating CSF Dynamics: In patients undergoing cranioplasty after decompressive craniectomy, FLAIR sequences help assess CSF flow patterns and potential areas of stagnation or hydrocephalus, which could impact postoperative recovery (Frontiers in Neurology, 2019).
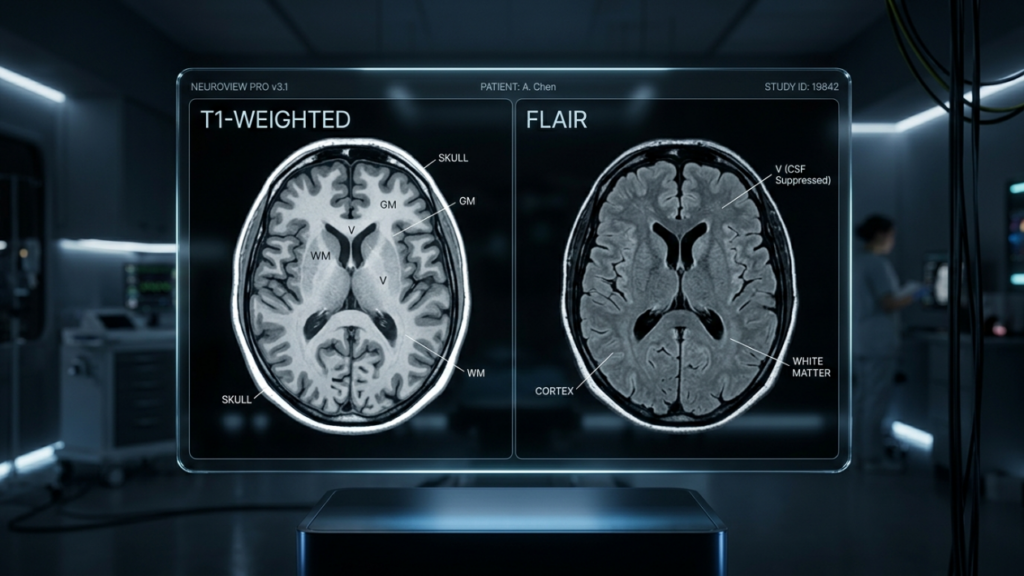
Comparative Analysis: T1 vs. FLAIR in Surgical Decision-Making
The choice between T1-weighted and FLAIR sequences is not binary but context-dependent. Surgeons often use both sequences in tandem to create a comprehensive preoperative map. Below is a comparative breakdown of their roles:
| Feature | T1-Weighted MRI | FLAIR MRI |
|---|---|---|
| Primary Use | Anatomical detail (bone, fat, hemorrhage) | Pathology detection (lesions, edema, CSF dynamics) |
| CSF Signal | Hyperintense (bright) | Suppressed (dark) |
| Cortical Bone | Hypointense (dark) | Hypointense (dark) |
| Lesion Detection | Limited near CSF | Enhanced near CSF |
| Clinical Application in Cranioplasty | Assessing bone integrity, fat-containing structures, and hemorrhage | Detecting periventricular lesions, brain parenchyma abnormalities, and CSF dynamics |
For example, a patient with a frontal bone defect and a history of trauma may require T1-weighted imaging to evaluate the bone’s structural integrity, while FLAIR sequences would be used to rule out underlying brain pathology that could complicate the cranioplasty procedure.
Clinical Case Study: Integrating T1 and FLAIR for Optimal Outcomes
Consider a 45-year-old male patient who underwent a decompressive craniectomy following a traumatic brain injury. Preoperative imaging revealed:
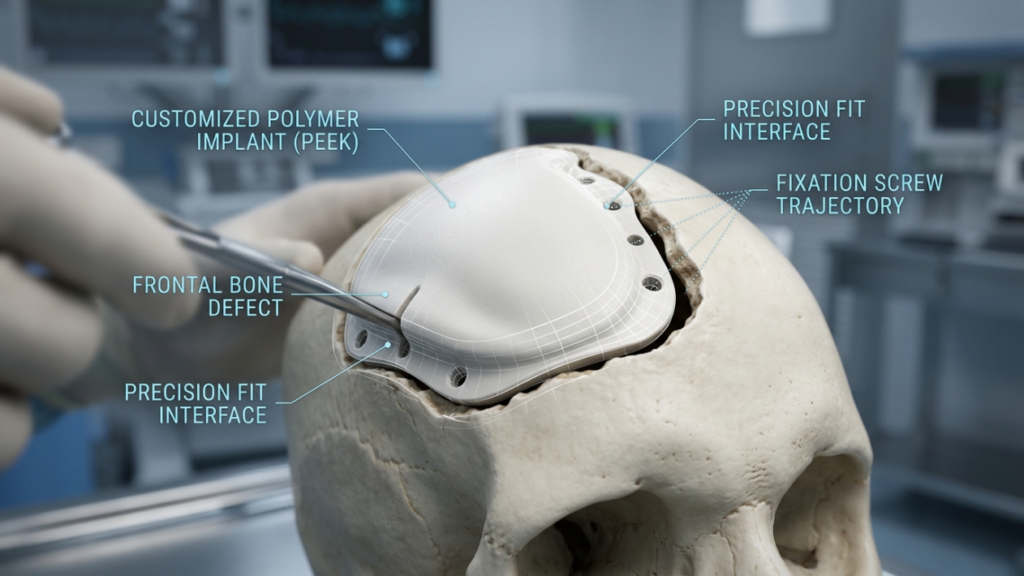
- T1-Weighted MRI: A large frontal bone defect with irregular margins, suggesting a complex fracture pattern. The cortical bone appeared hypointense, confirming the need for a customized synthetic implant.
- FLAIR MRI: Hyperintense lesions in the periventricular white matter, indicative of post-traumatic gliosis. These findings prompted the surgical team to opt for a delayed cranioplasty to allow for further neurological stabilization.
- Combined Insights: The integration of both sequences revealed that while the bone defect was suitable for reconstruction, the underlying brain pathology required additional monitoring to mitigate risks of postoperative seizures or CSF leaks.
Practical Steps for Surgeons: From Imaging to Implementation
To leverage T1 and FLAIR sequences effectively in cranioplasty planning, surgeons should follow these steps:
- Step 1: Preoperative Imaging Protocol
- Obtain both T1-weighted and FLAIR sequences as part of the standard MRI protocol.
- Ensure high-resolution images with thin slices (≤1 mm) for precise anatomical detail.
- Step 2: Bone and Brain Tissue Assessment
- Use T1-weighted images to evaluate the frontal bone’s structural integrity and identify any fat-containing lesions or hemorrhage.
- Use FLAIR images to assess brain parenchyma for lesions, edema, or gliosis that may impact surgical planning.
- Step 3: CSF Dynamics Evaluation
- Analyze FLAIR sequences for signs of CSF stagnation or hydrocephalus, which may necessitate additional interventions such as shunt placement.
- Step 4: Multidisciplinary Collaboration
- Consult with neuroradiologists to interpret subtle findings, particularly in cases with complex trauma or infection histories.
- Engage with neurosurgeons specializing in forehead contouring or facial reconstruction for insights on implant selection and placement.
- Step 5: Postoperative Monitoring
- Repeat MRI scans postoperatively to assess implant positioning and monitor for complications such as hematoma, infection, or CSF leaks.
Future Directions: Advancements in MRI Technology
The field of cranial radiology is evolving rapidly, with emerging technologies poised to further enhance cranioplasty planning:
- Zero Echo Time (ZTE) MRI: This technique offers superior visualization of cortical bone compared to traditional T1-weighted sequences, potentially improving the detection of subtle fractures or bone defects (Ultrashort Echo Time MRI, 2025).
- 3D FLAIR Sequences: Advanced 3D FLAIR imaging provides higher spatial resolution and reduced artifacts, enhancing the detection of periventricular lesions and CSF dynamics (3D-FLAIR in Neuroimaging, 2025).
- AI-Powered Image Analysis: Machine learning algorithms are being developed to automatically segment bone and brain tissue, reducing the time required for preoperative planning and improving accuracy (MRI-Based Bone Segmentation, 2025).

Frequently Asked Questions
Why is T1-weighted MRI preferred for assessing cortical bone in cranioplasty planning?
T1-weighted MRI is preferred because it provides high contrast between cortical bone (which appears hypointense) and surrounding soft tissues. This contrast allows surgeons to accurately assess bone integrity, fractures, and defects, which are critical for determining the feasibility of bone grafts or synthetic implants.
How does FLAIR MRI suppress CSF signal, and why is this important for cranioplasty?
FLAIR MRI uses an inversion recovery pulse to nullify the signal from cerebrospinal fluid (CSF). This suppression is crucial for cranioplasty because it enhances the visibility of periventricular lesions, brain parenchyma abnormalities, and areas of edema that might otherwise be obscured by the bright CSF signal on other sequences.
What are the limitations of T1-weighted MRI in cranioplasty planning?
The primary limitation of T1-weighted MRI is its inability to suppress CSF signal, which can obscure periventricular lesions or areas of edema near the frontal lobes. Additionally, it may not detect subtle brain parenchyma abnormalities as effectively as FLAIR sequences.
How do surgeons integrate T1 and FLAIR sequences in cranioplasty planning?
Surgeons use T1-weighted MRI to evaluate bone integrity and structural details, while FLAIR sequences are employed to detect brain pathology and CSF dynamics. By integrating both, they create a comprehensive preoperative map that guides implant selection, surgical approach, and postoperative monitoring.
What advancements in MRI technology are expected to impact cranioplasty planning?
Emerging technologies like Zero Echo Time (ZTE) MRI, 3D FLAIR sequences, and AI-powered image analysis are expected to enhance cranioplasty planning. ZTE MRI offers superior bone visualization, 3D FLAIR provides higher resolution for detecting lesions, and AI algorithms can automate segmentation and improve accuracy.
Why is CSF dynamics evaluation important in cranioplasty?
Evaluating CSF dynamics is critical because cranioplasty can alter CSF flow patterns. FLAIR sequences help identify areas of CSF stagnation or hydrocephalus, which may require additional interventions such as shunt placement to ensure optimal postoperative recovery and prevent complications.
What role does multidisciplinary collaboration play in cranioplasty planning?
Multidisciplinary collaboration ensures that surgeons, neuroradiologists, and specialists in facial reconstruction collectively interpret imaging findings. This collaboration is essential for addressing complex cases, optimizing implant selection, and mitigating risks associated with underlying brain pathology or CSF dynamics.



