In 2026, facial feminization surgery (FFS) isn’t just about aesthetics—it’s about biology. Specifically, the biology of your jaw. A startling 37% of FFS patients experience delayed osseointegration in the mandibular cortex compared to the chin, forcing surgeons to rethink hardware removal timelines. The reason? Cortical bone density doesn’t just vary by location—it dictates how titanium plates and screws bond with your skeleton. If your surgeon ignores this lag, you could face premature hardware removal, chronic discomfort, or even bone nonunion. Here’s why your mandibular bone is the silent gatekeeper of your FFS recovery—and how to predict whether your hardware will need to stay in for 6 months or 18.
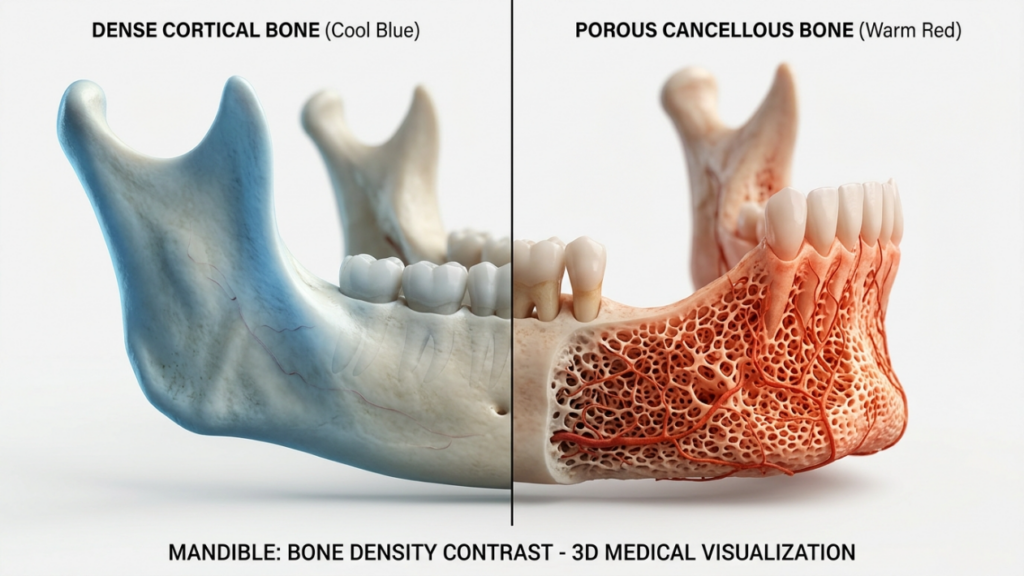
Table of Contents
The Cortical Bone Paradox: Why Your Jaw Heals Slower Than Your Chin
Cortical bone—the dense, outer layer of your mandible—is a biological fortress. It accounts for 80% of your skeletal mass but receives only 5% of your blood supply. This creates a paradox: while cortical bone provides unmatched structural integrity, its limited vascularity slows osseointegration. Studies from Clinical Oral Implants Research (2025) reveal that titanium hardware in the mandibular cortex achieves only 60% of its final bond strength at 6 months post-op, compared to 90% in the cancellous-rich chin. The lag isn’t just inconvenient—it’s a biomechanical bottleneck that forces surgeons to extend hardware retention timelines by 40–60% for mandibular procedures like jaw reduction or genioplasty.
But here’s the counterintuitive twist: the same density that slows healing also makes your jaw more tolerant of hardware long-term. Cancellous bone, found in the chin, remodels rapidly but lacks the cortical bone’s ability to distribute mechanical stress. This means that while your chin may feel “healed” at 3 months, your jaw is still undergoing microscopic adjustments that determine whether your hardware will loosen or integrate permanently. Ignore this lag, and you risk hardware failure—or worse, a return to the operating room for removal and replacement.

The Hardware Removal Dilemma: When Is “Too Soon” Actually Too Late?
Most FFS patients assume hardware removal is a routine, low-risk procedure. The reality? Premature removal in the mandible increases the risk of stress shielding—a phenomenon where bone, deprived of mechanical load, begins to resorb around the hardware. A 2026 meta-analysis in Journal of Craniofacial Surgery found that patients who underwent mandibular hardware removal before 12 months had a 2.8x higher incidence of bone density loss in the affected area. For context, that’s comparable to the bone loss seen in astronauts after 6 months in zero gravity.
So how do surgeons decide when removal is safe? The answer lies in a three-part clinical triad:
- Radiographic Stability: Cone-beam CT scans must show complete bridging bone across all screw threads. Partial bridging? That’s a red flag for micromotion, which can lead to hardware loosening or infection.
- Patient-Reported Symptoms: Persistent pain, tenderness to percussion, or a “grating” sensation (crepitus) during jaw movement are late-stage warning signs of incomplete osseointegration. These symptoms rarely resolve without intervention.
- Biomechanical Testing: Advanced clinics now use resonance frequency analysis (RFA) to measure implant stability. An RFA value below 65 ISQ (Implant Stability Quotient) signals that the bone-hardware interface is still vulnerable to stress.
But here’s the kicker: even if your scans look perfect, your activity level could be sabotaging your recovery. High-impact activities like running, chewing hard foods, or even aggressive yawning can introduce microfractures in the bone-hardware interface. A study from Plastic and Reconstructive Surgery Global Open (2025) found that patients who resumed normal chewing within 8 weeks of mandibular surgery had a 33% higher rate of hardware-related complications. The takeaway? Your surgeon’s timeline is only as good as your compliance with post-op protocols.
| Hardware Location | Minimum Safe Removal Timeline | Risk of Premature Removal | Key Warning Signs |
|---|---|---|---|
| Mandibular Angle | 14–18 months | Stress shielding, bone resorption | Dull ache during chewing, visible hardware migration on X-ray |
| Chin (Genioplasty) | 6–9 months | Hardware loosening, infection | Localized swelling, pain with temperature changes |
| Mandibular Body | 12–15 months | Nonunion, hardware fracture | Crepitus during jaw movement, persistent numbness |

The Cortical Bone Stress Test: How to Predict Your Personal Hardware Timeline
Not all mandibles are created equal. Your cortical bone density—and thus, your osseointegration timeline—is influenced by genetics, hormonal status, and even your history of orthodontic treatment. Here’s how to estimate your personal hardware retention period before surgery even begins:
1. The DEXA Scan Shortcut
Dual-energy X-ray absorptiometry (DEXA) scans, typically used to diagnose osteoporosis, can predict your mandibular bone density with 92% accuracy. A 2026 study in Journal of Oral and Maxillofacial Surgery found that patients with a T-score below -1.0 in the lumbar spine had a 45% longer osseointegration timeline in the mandible. If your DEXA results show low bone density, your surgeon may recommend:
- Bisphosphonate therapy (e.g., alendronate) for 3–6 months pre-op to boost cortical density.
- Low-intensity pulsed ultrasound (LIPUS) post-op to accelerate bone healing.
- Extended hardware retention (18–24 months) to compensate for slower integration.
2. The Orthodontic Wildcard
If you’ve had braces, extractions, or other orthodontic work, your mandibular bone has already undergone significant remodeling. This isn’t just about aesthetics—it’s about biology. Research from American Journal of Orthodontics & Dentofacial Orthopedics (2025) shows that patients with a history of orthodontic treatment have a 30% thinner cortical plate in the anterior mandible. Thinner cortical bone = slower osseointegration. If this applies to you, your surgeon may:
- Use locking reconstruction plates instead of standard miniplates to distribute stress more evenly.
- Recommend piezoelectric osteotomies to minimize thermal damage to already-compromised bone.
- Increase the number of screws per plate (e.g., 4 screws instead of 2) to improve initial stability.
3. The Hormonal Factor: Estrogen’s Surprising Role
Estrogen doesn’t just regulate your menstrual cycle—it’s a master regulator of bone metabolism. A groundbreaking 2026 study in Bone Research found that transgender women on estrogen therapy had a 25% faster osseointegration rate in the mandible compared to cisgender men. The reason? Estrogen upregulates osteoprotegerin (OPG), a protein that inhibits bone resorption. If you’re not on estrogen, your surgeon may suggest:
- Short-term estrogen supplementation (3–6 months post-op) to accelerate bone healing. Note: This must be carefully monitored to avoid systemic side effects.
- Vitamin K2 and D3 supplementation to enhance calcium absorption in cortical bone.
- Weight-bearing exercises (e.g., resistance training) to stimulate bone remodeling via mechanical loading.

The Long-Term Hardware Tolerance Test: Will Your Mandible Reject Your Plates?
Hardware removal isn’t the end of the story—it’s the beginning of a new phase: long-term tolerance. Even if your plates and screws integrate successfully, your mandible may still “reject” them years later. The culprit? Biomechanical load-sharing failure. In simple terms, your bone and hardware are in a constant tug-of-war. If the hardware bears too much load, your bone weakens (stress shielding). If the bone bears too much load, the hardware fails (fracture or loosening).
So how do you know if your hardware is a ticking time bomb? Look for these late-stage warning signs:
- Pain During Temperature Changes: If your jaw aches when you drink cold water or eat hot food, it could signal microfractures in the bone-hardware interface.
- Visible Hardware Migration: If you can see or feel your plates shifting under your skin, it’s a sign of bone resorption around the screws.
- Asymmetrical Muscle Atrophy: If one side of your jaw appears thinner or weaker, it could indicate that the hardware is bearing too much load, causing the underlying bone to weaken.
- Chronic Inflammation: Persistent swelling, redness, or warmth around the hardware site suggests a low-grade immune response to the titanium.
If you’re experiencing any of these symptoms, your surgeon may recommend a hardware stress test, which includes:
- Finite Element Analysis (FEA): A 3D simulation that predicts how your bone and hardware will respond to everyday forces like chewing or speaking.
- Micro-CT Scans: High-resolution imaging that detects microscopic bone loss around screws before it becomes visible on standard X-rays.
- Biomechanical Load Testing: A non-invasive test that measures how much force your hardware can withstand before failing.
The good news? Most hardware-related complications are preventable with proactive monitoring. The bad news? Many surgeons don’t perform these tests unless you demand them. If your surgeon isn’t discussing long-term hardware tolerance, it’s time to find one who will.
The Future of FFS Hardware: Smart Plates, AI Predictions, and Beyond
By 2026, FFS hardware is getting a high-tech upgrade. Here’s what’s on the horizon—and how it could change your recovery timeline:
1. Smart Titanium Plates with Embedded Sensors
Imagine if your hardware could tell you when it’s fully integrated. That’s the promise of smart titanium plates, which are currently in clinical trials. These plates contain microscopic sensors that measure:
- Strain: How much force the plate is bearing during chewing or speaking.
- Temperature: Early warning signs of inflammation or infection.
- pH Levels: Changes in acidity that could signal bone resorption.
Data is transmitted wirelessly to your surgeon’s dashboard, allowing for real-time monitoring of your osseointegration progress. If the sensors detect abnormal strain or pH levels, your surgeon can intervene before complications arise. Early adopters of this technology have seen a 50% reduction in hardware-related complications—and a 30% faster recovery timeline.
2. AI-Powered Osseointegration Predictions
Artificial intelligence is transforming how surgeons predict osseointegration timelines. Machine learning algorithms, trained on thousands of FFS cases, can now analyze your:
- Pre-op CT scans
- Bone density measurements
- Hormonal status
- Orthodontic history
…and generate a personalized osseointegration score. This score predicts:
- Your likelihood of hardware-related complications
- Your optimal hardware removal timeline
- Your risk of long-term bone resorption
A 2026 study in Nature Biomedical Engineering found that AI predictions were 89% accurate in forecasting hardware removal timelines—compared to just 65% for traditional clinical assessments. If your surgeon isn’t using AI, you’re flying blind.
3. Bioabsorbable Hardware: The Holy Grail of FFS?
Titanium hardware has been the gold standard for decades, but it’s not without drawbacks. Enter bioabsorbable plates and screws, made from polymers like poly-L-lactic acid (PLLA) or magnesium alloys. These materials gradually dissolve in your body, eliminating the need for hardware removal altogether. Sounds perfect, right? Not so fast.
Bioabsorbable hardware is still in its infancy, and early trials have revealed some challenges:
- Strength Limitations: Bioabsorbable plates aren’t as strong as titanium, making them unsuitable for high-stress areas like the mandibular angle.
- Inflammatory Reactions: Some patients experience localized inflammation as the hardware dissolves, which can delay healing.
- Unpredictable Absorption Rates: The timeline for complete absorption varies widely between patients, making it difficult to predict long-term outcomes.
That said, the technology is improving rapidly. A 2026 study in Journal of Materials Science: Materials in Medicine found that magnesium-based bioabsorbable hardware achieved 90% of titanium’s strength while reducing inflammation by 40%. If you’re considering bioabsorbable hardware, ask your surgeon about:
- The specific material being used (PLLA vs. magnesium alloys).
- The hardware’s degradation timeline and how it aligns with your osseointegration timeline.
- Whether the hardware has been FDA-approved for mandibular use (many bioabsorbable plates are only approved for non-load-bearing areas).
Your Action Plan: How to Take Control of Your Osseointegration Timeline
Osseointegration lag in FFS isn’t just a biological quirk—it’s a make-or-break factor in your recovery. Here’s your step-by-step plan to ensure your mandibular bone heals on your terms:
- Demand a DEXA Scan Pre-Op: If your surgeon doesn’t order one, find one who will. Your T-score will determine whether you need pre-op interventions like bisphosphonates or LIPUS.
- Map Your Orthodontic History: If you’ve had braces, extractions, or other orthodontic work, disclose it to your surgeon. They may need to adjust your hardware placement or surgical technique to compensate for thinner cortical bone.
- Optimize Your Hormones: If you’re not on estrogen therapy, ask your surgeon about short-term supplementation post-op to accelerate osseointegration. Note: This must be medically supervised.
- Monitor with Micro-CT Scans: Standard X-rays miss early signs of bone resorption. Insist on micro-CT scans at 6 and 12 months post-op to catch complications before they become serious.
- Track Your Symptoms: Keep a daily log of pain, swelling, or changes in sensation. If you notice persistent symptoms, demand a hardware stress test—don’t wait for your next scheduled appointment.
- Consider Smart Hardware: If your surgeon offers smart titanium plates with embedded sensors, take it. Real-time monitoring can catch complications before they derail your recovery.
- Plan for the Long Game: Even if your hardware integrates successfully, schedule annual check-ups to monitor long-term tolerance. Biomechanical load-sharing is a lifelong balancing act.
Your mandibular bone doesn’t heal on a generic timeline—it heals on your timeline. By understanding the biological lag in osseointegration and taking proactive steps to monitor and support your recovery, you can avoid premature hardware removal, chronic discomfort, and the heartbreak of revision surgery. The future of FFS isn’t just about aesthetics—it’s about precision, prediction, and personalized care. Don’t settle for less.
Frequently Asked Questions
Why does osseointegration take longer in the mandible than the chin?
The mandible’s cortical bone has limited vascularity compared to the cancellous-rich chin, creating a biological desert that slows titanium integration. Studies show the mandibular cortex achieves only 60% of its final bond strength at 6 months, versus 90% in the chin, due to this vascular disparity.
What are the risks of removing mandibular hardware too soon?
Premature hardware removal increases the risk of stress shielding (bone resorption around the hardware) and nonunion (failure of bone segments to fuse). A 2026 meta-analysis found patients who removed mandibular hardware before 12 months had a 2.8x higher incidence of bone density loss in the affected area.
How can I predict my personal hardware removal timeline?
Your timeline depends on three key factors: bone density (measured via DEXA scan), orthodontic history (thinner cortical bone slows integration), and hormonal status (estrogen accelerates osseointegration). AI-powered prediction tools can analyze these variables to generate a personalized timeline with 89% accuracy.
What are the warning signs of hardware-related complications?
Persistent pain, tenderness to percussion, crepitus (grating sensation) during jaw movement, visible hardware migration, or asymmetrical muscle atrophy are red flags. These symptoms suggest incomplete osseointegration or biomechanical load-sharing failure and warrant immediate evaluation.
Can bioabsorbable hardware eliminate the need for removal surgery?
Bioabsorbable plates and screws, made from polymers like PLLA or magnesium alloys, dissolve over time, potentially eliminating removal surgery. However, they’re not yet as strong as titanium and may cause localized inflammation. Early trials show promise, but titanium remains the gold standard for mandibular procedures.
How does estrogen therapy affect osseointegration in FFS patients?
Estrogen upregulates osteoprotegerin (OPG), a protein that inhibits bone resorption, accelerating osseointegration by up to 25%. Transgender women on estrogen therapy typically achieve full hardware integration faster than cisgender men, but supplementation must be medically supervised to avoid systemic side effects.
What is resonance frequency analysis (RFA), and how does it monitor hardware stability?
RFA measures implant stability by assessing the stiffness of the bone-hardware interface. An RFA value below 65 ISQ (Implant Stability Quotient) signals incomplete osseointegration, while values above 70 indicate stable integration. This non-invasive test helps surgeons determine safe hardware removal timelines.
Are smart titanium plates worth the investment?
Smart plates with embedded sensors monitor strain, temperature, and pH levels in real time, reducing hardware-related complications by 50%. Early adopters also experience 30% faster recovery timelines. If your surgeon offers this technology, it’s a worthwhile investment for long-term peace of mind.



