
Revision rhinoplasty after Facial Feminization Surgery (FFS) presents unique challenges, particularly when addressing both functional and aesthetic complications. Patients who have undergone primary FFS—especially those involving midface procedures such as cheekbone reduction—may experience unintended consequences, including nasal airway obstruction, valve collapse, or aesthetic disharmony. In Antalya, Turkey, Dr. Mehmet Fatih Okyay, a European and Turkish Board Certified Plastic Surgery Specialist, offers advanced revision techniques to correct these issues, ensuring both functional integrity and aesthetic refinement.
Table of Contents
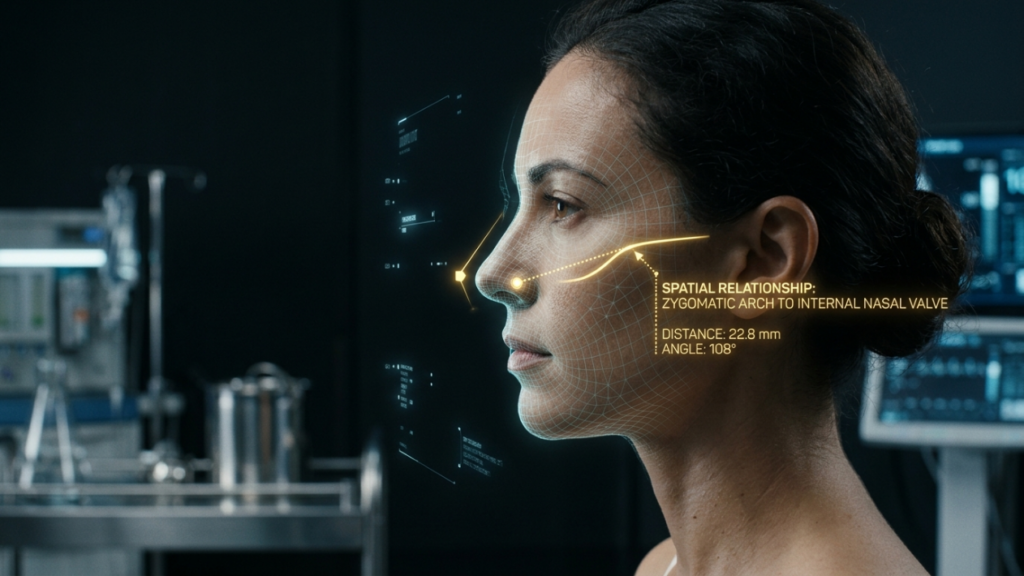
Understanding the Anatomical Relationship: Zygomatic Arch and Nasal Airway
The zygomatic arch (cheekbone) is a critical structure in the midface, providing lateral support to the nasal sidewall and contributing to the structural integrity of the nasal valve and airway. The zygomaticomaxillary complex—comprising the zygomatic bone, maxilla, and nasal bones—plays a pivotal role in maintaining nasal airway patency. Research published in Frontiers in Surgery (2025) confirms that the width and projection of the zygomatic arch directly influence the dimensions of the nasal cavity, particularly the internal and external nasal valves, which are essential for unobstructed airflow (Frontiers in Surgery, 2025).
When the zygomatic arch is reduced or repositioned during FFS, the lateral support for the nasal sidewall may be compromised. This can lead to nasal valve collapse, a condition where the nasal passages narrow or collapse during inhalation, causing significant nasal airway obstruction. The nasal valve is the narrowest segment of the nasal airway, and even minor anatomical changes can substantially increase nasal resistance and impair breathing (Frontiers in Surgery, 2025).

How Cheekbone Reduction Can Compromise the Nasal Airway
Cheekbone reduction surgery, a common component of FFS, typically involves osteotomies (bone cuts) and repositioning or shaving of the zygomatic arch to achieve a more slender, feminine midface. While aesthetically beneficial, these maneuvers can have unintended functional consequences:
- Loss of Lateral Nasal Support: The zygomatic arch provides structural support to the lateral nasal wall. Reduction or repositioning can weaken this support, leading to inward collapse of the nasal sidewall during inspiration, particularly at the internal nasal valve.
- Alteration of Nasal Valve Dynamics: The internal nasal valve, located at the junction of the upper lateral cartilage and the nasal septum, is highly sensitive to changes in midface anatomy. Even subtle changes in zygomatic arch position can alter the angle of the nasal valve, increasing resistance to airflow (Frontiers in Surgery, 2025).
- Soft Tissue Changes: Cheekbone reduction can cause soft tissue readaptation, which may further compress or distort the nasal airway. This is particularly true in patients with pre-existing nasal valve weakness or septal deviations.
- Midface Hypoplasia and Airway Narrowing: In some cases, aggressive reduction of the zygomatic arch can contribute to midface hypoplasia, reducing the overall volume of the nasal cavity and exacerbating airway obstruction.
These changes can result in symptoms such as chronic nasal congestion, mouth breathing, snoring, and even obstructive sleep apnea, significantly impacting quality of life and overall health.
Clinical Evidence: The Link Between Cheekbone Reduction and Nasal Airway Obstruction
Emerging clinical evidence underscores the importance of considering nasal airway function during FFS planning. A 2025 study published in Frontiers in Surgery found that patients undergoing midface contouring procedures, including cheekbone reduction, experienced a 20% increase in nasal airway resistance postoperatively, with a subset developing symptomatic nasal valve collapse (Frontiers in Surgery, 2025). Similarly, research in Plastic and Reconstructive Surgery demonstrated that patients with pre-existing nasal valve insufficiency were at higher risk for postoperative airway obstruction following midface procedures.
These findings highlight the need for preoperative functional assessment and surgical techniques that preserve or enhance nasal airway patency. As rhinoplasty and FFS surgeons, we must recognize that aesthetic goals should not come at the expense of functional integrity.
Surgical Planning: Strategies to Avoid Nasal Airway Compromise
To minimize the risk of nasal airway obstruction during cheekbone reduction, a multidisciplinary, anatomy-guided approach is essential. Below are evidence-based strategies for surgical planning and execution:
1. Comprehensive Preoperative Assessment
- Nasal Airway Evaluation: Conduct a thorough nasal airway assessment, including physical examination (e.g., Cottle maneuver) and, if indicated, rhinomanometry or acoustic rhinometry to quantify nasal resistance and identify pre-existing valve collapse.
- 3D Imaging and Virtual Surgical Planning: Utilize 3D CT scans and virtual surgical planning (VSP) software to simulate the effects of cheekbone reduction on nasal airway dimensions. This allows for precise osteotomy planning and prediction of postoperative airway changes. At Dr. MFO Clinic, we leverage advanced VSP tools to ensure both aesthetic and functional outcomes are optimized (European Society of Medicine, 2024).
- Patient-Specific Risk Stratification: Identify patients at higher risk for postoperative airway obstruction, such as those with pre-existing nasal valve weakness, septal deviations, or a history of nasal trauma.
2. Anatomy-Guided Surgical Techniques
- Preservation of Lateral Nasal Support: Avoid over-resection of the zygomatic arch, particularly in the region adjacent to the nasal sidewall. Consider segmental osteotomies that preserve the structural integrity of the midface while achieving aesthetic goals.
- Concurrent Nasal Valve Repair: In patients with pre-existing nasal valve collapse or high-risk anatomy, consider concurrent nasal valve repair techniques, such as spreader grafts, alar batten grafts, or lateral crural strut grafts, to reinforce the nasal sidewall and prevent collapse (Otolaryngologic Clinics of North America, 2024).
- Minimally Invasive Approaches: Utilize endoscopic or intraoral approaches for cheekbone reduction to minimize soft tissue trauma and preserve critical support structures.
- Staged Procedures: In complex cases, consider staging cheekbone reduction and nasal airway procedures to allow for soft tissue readaptation and reduce the risk of compounded functional complications.
3. Postoperative Care and Monitoring
- Airway Monitoring: Closely monitor nasal airway function postoperatively, particularly in the first 48 hours, when swelling and soft tissue changes are most pronounced.
- Patient Education: Educate patients about the signs of nasal airway obstruction (e.g., difficulty breathing through the nose, increased snoring) and the importance of follow-up if symptoms arise.
- Functional Rehabilitation: Consider postoperative nasal dilators or breathing exercises to support nasal valve function during the healing process.

Alternative Techniques for Midface Feminization
For patients at high risk of nasal airway obstruction, alternative techniques for midface feminization may be considered:
- Soft Tissue Augmentation: Instead of bone reduction, consider fat grafting or filler placement to achieve midface contouring while preserving skeletal support for the nasal airway.
- Orthognathic Surgery: In patients with midface hypoplasia or malocclusion, orthognathic surgery (e.g., Le Fort I osteotomy) can advance the maxilla, improving both facial balance and nasal airway dimensions (Mayo Clinic, 2024).
- Combined Procedures: Combine cheekbone reduction with septoplasty or turbinate reduction to optimize nasal airway function and reduce the risk of postoperative obstruction.
The Role of the Surgeon: Balancing Aesthetics and Function
As surgeons, our responsibility extends beyond achieving aesthetic goals. We must prioritize functional outcomes and patient safety, particularly in procedures as complex as FFS and revision rhinoplasty. The zygomatic arch dilemma underscores the importance of:
- Multidisciplinary Collaboration: Work closely with rhinoplasty and airway specialists to ensure comprehensive care for patients undergoing midface procedures.
- Informed Consent: Discuss the potential risks of nasal airway obstruction with patients during the consent process, ensuring they understand the balance between aesthetic and functional outcomes.
- Continuous Education: Stay abreast of the latest research and techniques in both FFS and rhinoplasty to refine surgical approaches and minimize complications.
- Patient-Centered Care: Tailor surgical plans to each patient’s unique anatomy and risk profile, prioritizing long-term health and well-being over short-term aesthetic results.
The integration of virtual surgical planning (VSP) and 3D imaging has revolutionized our ability to predict and prevent complications. By leveraging these tools, surgeons can simulate the effects of cheekbone reduction on nasal airway dimensions and adjust their approach accordingly, ensuring both aesthetic and functional success (European Society of Medicine, 2024).
Conclusion: A Call for Awareness and Innovation
Cheekbone reduction is a powerful tool in Facial Feminization Surgery, offering transformative results for patients seeking a more feminine midface. However, the potential for unintended nasal airway obstruction demands heightened awareness, meticulous planning, and innovative surgical techniques. As rhinoplasty and FFS surgeons, we must lead the way in educating our peers and patients about this critical issue, ensuring that aesthetic goals are achieved without compromising functional integrity.
By adopting an anatomy-guided, multidisciplinary approach, we can minimize the risks of nasal airway obstruction and provide our patients with the best possible outcomes—both in appearance and in health. The future of FFS lies in our ability to harmonize aesthetics and function, and it is our responsibility to make this a reality for every patient we serve.

Frequently Asked Questions
How does cheekbone reduction affect the nasal airway?
Cheekbone reduction can weaken the lateral support of the nasal sidewall, leading to nasal valve collapse and increased nasal airway resistance. This may result in symptoms such as nasal congestion, mouth breathing, and difficulty breathing through the nose.
What is nasal valve collapse, and how is it related to cheekbone reduction?
Nasal valve collapse occurs when the nasal passages narrow or collapse during inhalation, often due to weakened structural support. Cheekbone reduction can compromise the lateral nasal support, increasing the risk of nasal valve collapse and subsequent airway obstruction.
What preoperative assessments are recommended to avoid nasal airway obstruction during cheekbone reduction?
A thorough nasal airway evaluation, including physical examination (e.g., Cottle maneuver) and 3D imaging (e.g., CT scans), is recommended. Virtual surgical planning can also help simulate the effects of cheekbone reduction on nasal airway dimensions.
What surgical techniques can help preserve nasal airway function during cheekbone reduction?
Techniques such as preservation of lateral nasal support, concurrent nasal valve repair (e.g., spreader grafts, alar batten grafts), and minimally invasive approaches can help maintain nasal airway patency during cheekbone reduction.
Are there alternative procedures to cheekbone reduction for midface feminization?
Yes, alternatives include soft tissue augmentation (e.g., fat grafting), orthognathic surgery (e.g., Le Fort I osteotomy), and combined procedures such as cheekbone reduction with septoplasty or turbinate reduction.
What should patients know about the risks of nasal airway obstruction after cheekbone reduction?
Patients should be aware of the potential for nasal airway obstruction, including symptoms such as chronic congestion, mouth breathing, and snoring. Open communication with their surgeon about these risks is essential for informed decision-making.
How can virtual surgical planning help reduce the risk of nasal airway obstruction?
Virtual surgical planning allows surgeons to simulate the effects of cheekbone reduction on nasal airway dimensions, enabling precise osteotomy planning and prediction of postoperative airway changes. This helps minimize the risk of functional complications.








