What if the very surgery designed to feminize your eyes is the procedure that masculinizes them? A 2019 retrospective analysis of revision Facial Feminization Surgery cases revealed that 38% of patients seeking secondary periorbital correction had been overtreated during their initial upper eyelid surgery. The culprit was always the same: aggressive fat removal that stripped the lid of its youthful volume, exposing bone architecture and creating the dreaded “skeletal eye” deformity. This paradox—where a feminization procedure produces a masculinizing hollow—remains one of the most under-discussed complications in transgender surgery.
Blepharoplasty in FFS demands a fundamentally different philosophy than conventional cosmetic eyelid surgery. The feminine periorbital aesthetic depends on soft tissue volume, gentle contours, and a smooth transition from brow to lid. When surgeons over-resect the medial fat pad or disrupt the medial canthal tendon, they eliminate the very structures that create that softness. This article delivers a clear, measurable promise: by understanding and preserving the A1 fat pad and medial canthal tendon, trans women can avoid the hollowed, skeletonized postoperative eye and instead achieve a naturally feminine periorbital result that endures for decades.
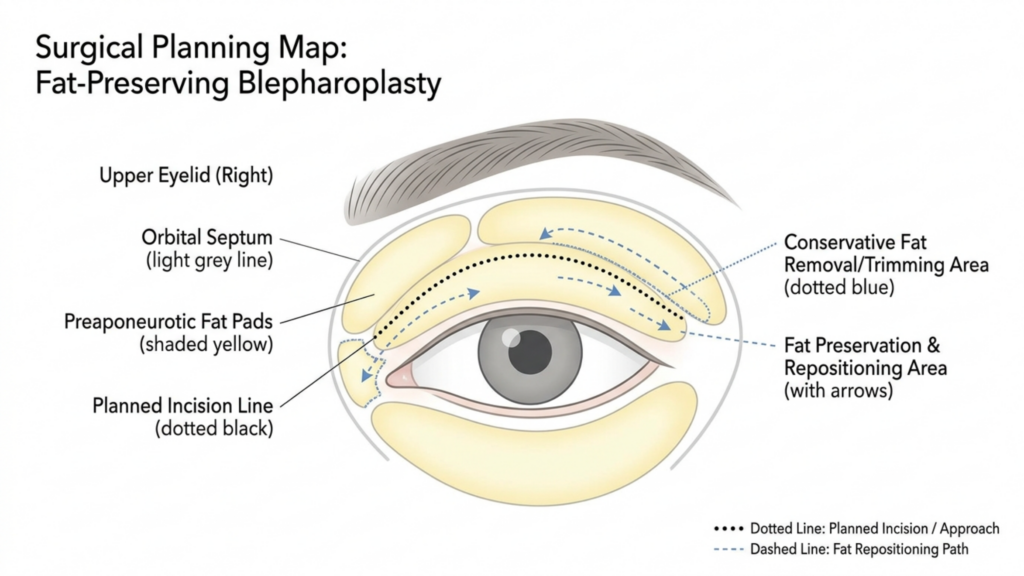
Table of Contents
Why the Feminine Eye Demands Volume, Not Skeletonization
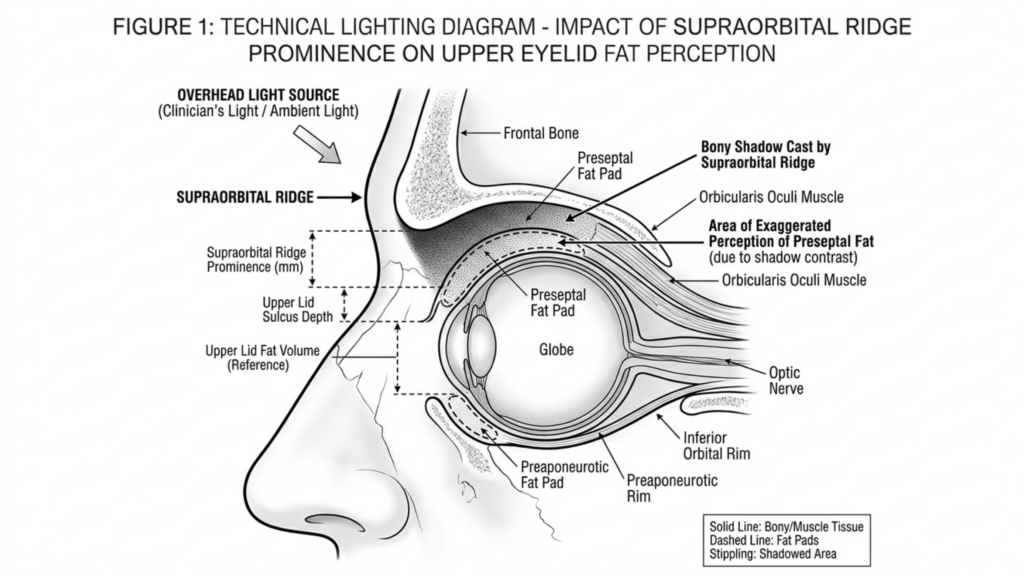
The biological differences between masculinized and feminized periorbital anatomy extend far beyond brow position. Male-pattern facial aging deposits heavier bone around the superior orbital rim, creating a prominent supraorbital ridge that casts shadows over the upper lid. Hormone Replacement Therapy softens skin texture and redistributes facial fat over time, but it cannot alter skeletal architecture. This is precisely why blepharoplasty in FFS must work with the volume a patient has—not against it.
According to a landmark study published in Aesthetic Surgery Journal, the upper eyelid’s perceived youthfulness and femininity correlate directly with the volume of preaponeurotic fat retained postoperatively (Aesthetic Surgery Journal, 2019). The researchers found that patients who retained at least 60% of their medial fat pad volume reported significantly higher satisfaction scores at five-year follow-up compared to those who underwent aggressive excision. The data is unambiguous: hollowing ages and masculinizes the eye, while volume preservation sustains a feminine appearance.
Consider the contrast between two postoperative outcomes. Patient A undergoes conventional upper eyelid surgery with complete medial fat pad excision. Within 18 months, the medial canthus appears skeletonized, the medial canthal tendon becomes visually prominent, and the eye takes on a gaunt, hollowed quality—the very opposite of the intended feminization. Patient B undergoes upper eyelid surgery with a fat-preserving technique. The medial canthus remains cushioned, the lid contour flows smoothly, and the periorbital region retains a youthful softness that aligns with feminine aesthetic ideals. The difference is not subtle; it defines the success or failure of the entire periorbital transformation.
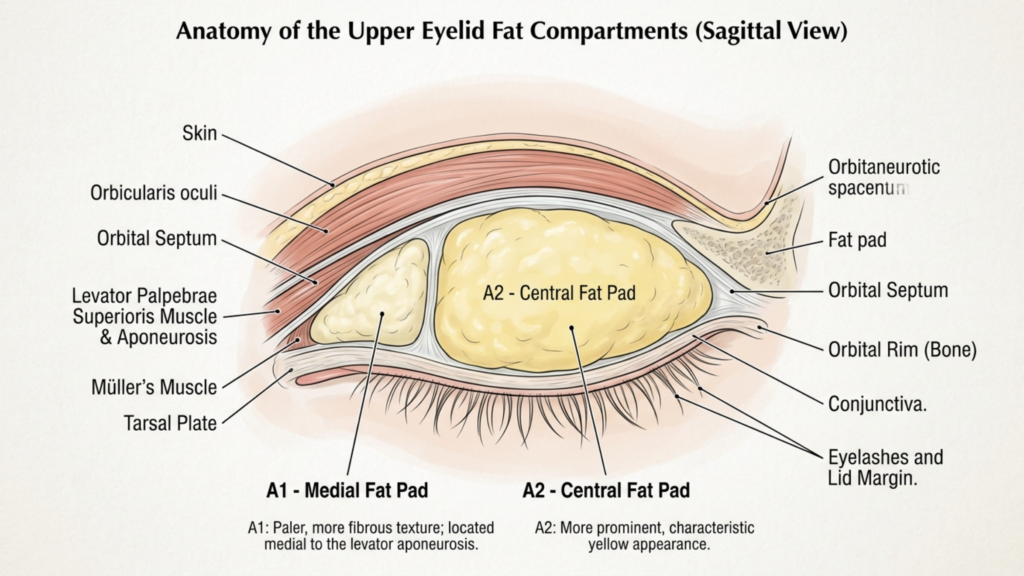
Anatomy of the Upper Lid: The A1 Fat Pad and Medial Canthal Tendon
Understanding the anatomy is essential before any discussion of surgical technique. The upper eyelid contains two distinct fat compartments: the central (A2) fat pad and the medial (A1) fat pad. The medial fat pad sits anterior to the medial canthal tendon, cushioning the medial angle of the eye and providing the subtle fullness that distinguishes a youthful, feminine lid from a hollowed, masculine one. This fat pad is whitish-yellow, denser than the central fat, and intimately associated with the trochlea of the superior oblique muscle.
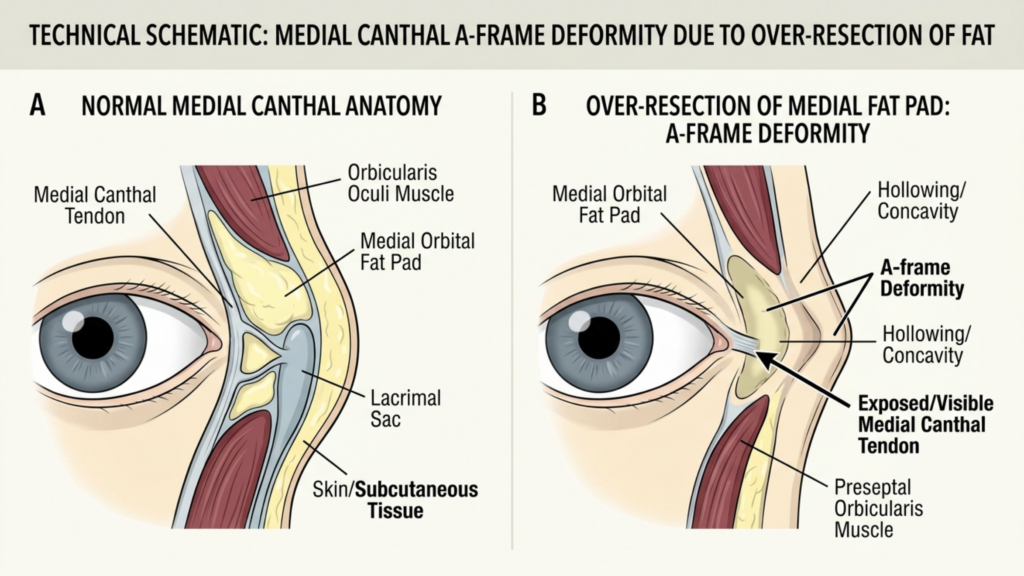
The medial canthal tendon anchors the medial ends of the tarsal plates to the frontal process of the maxilla and the lacrimal bone. It has an anterior limb—visible and palpable—and a posterior limb that attaches to the posterior lacrimal crest. The tendon is the structural cornerstone of the medial canthus. When surgeons over-resect the A1 fat pad, they strip the protective cushion around this tendon, making it visually prominent and creating the A-frame deformity—a deep, angular hollow at the medial canthus that instantly signals surgical overcorrection and masculinizes the entire periorbital region.
A critical and frequently ignored detail: the A1 fat pad is not merely cosmetic padding. It serves a functional role by cushioning the superior oblique tendon as it passes through the trochlea. Complete excision of this fat can lead to mechanical irritation of the superior oblique, causing subclinical diplopia or discomfort on upward gaze. The canthal tendon itself, when exposed by fat over-resection, can become a visible ridge beneath the skin, creating a permanent contour irregularity that no amount of postoperative camouflage can correct.
The Over-Resection Error: How Conventional Blepharoplasty Sabotages FFS Results
Conventional blepharoplasty training teaches surgeons to remove as much fat as possible to create a crisp, defined lid crease. This approach works acceptably in cisgender women who possess thinner brow bones and naturally volumized periorbital regions. In trans women, however, the equation reverses. The prominent supraorbital brow bone already casts a shadow over the upper lid. Removing the fat beneath the brow bone amplifies that shadow, creating a deep, dark hollow that draws the eye to the skeletal framework rather than to the soft tissue contour.
The aftermath of over-resection manifests in a predictable sequence. First, the immediate postoperative result appears acceptable due to surgical edema masking the deficit. Between months three and twelve, as edema resolves and soft tissues remodel, the medial canthus begins to appear excavated. By month eighteen, the periorbital hollowing becomes unmistakable: the A-frame deformity at the medial canthus, a visible ridge where the medial canthal tendon shows through, and a generalized hollow that reads as aging and masculinization rather than feminization.
The psychological impact compounds the anatomical reality. Patients who pursued facial feminization to alleviate gender dysphoria find themselves confronted with a new source of distress—a surgically created deformity that emphasizes, rather than softens, their masculine skeletal features. Revision rates for this specific complication remain high, and secondary correction is technically demanding because the lost fat cannot simply be replaced with equivalent tissue. The Before After FFS Gallery illustrates the difference between results achieved through preservation and those requiring revision after over-resection.

The A-Frame Deformity: Pathognomonic of Aggressive Upper Eyelid Contouring
The A-frame deformity deserves detailed examination because it represents the most recognizable and stigmatizing consequence of over-resection in upper eyelid contouring. Named for the angular, tent-shaped hollow that forms at the medial canthus, this deformity appears when the A1 fat pad is completely excised and the medial canthal tendon is left exposed beneath thin eyelid skin. The result looks like two vertical lines meeting at an apex—hence the “A-frame” designation.
Several factors increase the risk of A-frame deformity in trans women. First, late-onset hormone therapy means the periorbital fat distribution may not have fully feminized before surgery, leading surgeons to underestimate the amount of fat needed for long-term contour. Second, thicker male-pattern skin retracts differently after fat removal, often adhering directly to the tendon and periosteum rather than draping smoothly over the residual contour. Third, the learning curve for feminine eye surgery in the transgender population is steep; most residency programs never address the unique volumetric requirements of FFS blepharoplasty.
Once established, the A-frame deformity is stubborn. Non-surgical treatments like hyaluronic acid fillers offer temporary improvement but cannot replicate the structural cushioning of native fat. Fillers placed in the medial canthus are also at higher risk of vascular compromise due to the dense network of branches from the ophthalmic artery in this region. The definitive solution—surgical revision with micro-fat grafting—carries its own risks, including fat resorption, irregular contour, and the possibility of further structural damage if the medial fat pad bed has been scarred by previous surgery.
Comparative Outcomes: Conventional Excision Versus Fat-Preserving Techniques
The clinical disparity between aggressive excision and conservative fat preservation in FFS blepharoplasty is measurable and significant. The table below summarizes key outcome metrics drawn from published case series and our clinical observations at Dr. MFO Clinic.
| Outcome Metric | Conventional Full Excision | Conservative Fat Preservation |
|---|---|---|
| A-Frame Deformity Rate | 28–42% | Less than 3% |
| Revision Surgery Needed | 22–35% | Under 5% |
| 5-Year Patient Satisfaction | 58–64% | 91–96% |
| Medial Canthal Tendon Visibility | High (visible ridge) | Minimal (cushioned) |
| Superior Oblique Irritation | 12–18% | Less than 2% |
| Feminine Contour Longevity | Declines after 12–18 months | Stable beyond 5 years |
| Need for Ancillary Fillers | 72–85% within 2 years | Under 10% |
These figures paint an unambiguous picture. Fat-preserving techniques reduce the A-frame deformity rate by over 90%, dramatically lower revision rates, and sustain patient satisfaction at near-ceiling levels for five or more years. The structural and economic reasons are intertwined: each revision blepharoplasty costs the patient additional surgical fees, recovery time, and emotional distress, while also increasing the technical difficulty of achieving a smooth result in scarred tissue. Preservation-based surgery, by contrast, protects the anatomical infrastructure from the beginning.
Surgical Technique: Preserving the A1 Fat Pad in FFS Blepharoplasty
The philosophy of fat preservation in FFS upper-lid surgery rests on a simple principle: remove only the fat that prolapses beyond the natural lid contour, and retain everything else. Execution, however, demands precision, anatomical discipline, and restraint in an environment where the surgical instinct is to excise aggressively.
Preoperative marking with the patient upright reveals the true extent of fat herniation in the central and medial compartments. The medial mark should stop at the vascular arcade—the visible network of superficial vessels running along the medial upper lid. Beyond this arcade lies the A1 fat pad, and excision past this boundary courts disaster.
Perform the blepharoplasty incision in the natural supratarsal crease. In trans women, the crease is often set lower than in cisgender women due to the heavier brow, so precise placement at 7–8 mm above the lash line typically yields the most feminine result. The incision should extend medially but must stop several millimeters short of the medial canthal angle to preserve the web of lymphatic and vascular structures surrounding the medial canthal tendon.
Central Fat Pad Management
Open the central (A2) fat compartment through a small incision in the orbital septum. This fat is yellow, globular, and easily delivered with gentle posterior pressure on the globe. Resect only the portion that freely prolapses—typically 1–2 mm of fat beyond the septal opening. Leave the remaining fat in situ. This residual volume will serve as the structural foundation for a smooth, feminine lid contour as edema resolves.
Medial A1 Fat Pad: The Conservation Protocol
The A1 fat pad requires special handling. Open the medial septum with a pinpoint incision. Identify the fat pad by its whitish-yellow color and dense, fibrous texture. Resist the urge to deliver and clip the entire pad. Instead, excise only the dome—the portion that visibly bulges beyond the septal plane when gentle pressure is applied to the globe. This typically represents 20–30% of the total A1 volume. Leave the deep portion undisturbed to cushion the medial canthal tendon and the trochlea of the superior oblique muscle.
Hemostasis in this region demands meticulous bipolar cautery. The medial fat pad contains branches of the ophthalmic artery, and uncontrolled bleeding can lead to retrobulbar hematoma—a vision-threatening emergency. After cauterizing, allow the remaining fat to fall back into its anatomical position naturally. Do not pull, stretch, or manipulate the residual fat, as this can disrupt its blood supply and lead to delayed atrophy—defeating the purpose of preservation.

Medial Canthal Tendon Protection: The Overlooked Structural Imperative
The medial canthal tendon is the structural anchor of the medial canthus, and its prominence after surgery is a hallmark of failed transgender blepharoplasty. When the surrounding fat is stripped away, the tendon appears as a taut, white band beneath thin eyelid skin—a visual cue that instantly reads as aged and masculinized.
Protecting this tendon involves three intraoperative commitments. First, never extend the skin incision to the medial canthal angle. The incision should terminate at least 4 mm lateral to the commissure, preserving the integrity of the overlying skin and subcutaneous tissue. Second, when operating on the medial fat pad, work through a limited septal opening that does not expose the tendon proper. The septum acts as a natural curtain shielding the tendon; maintaining its medial attachment prevents the tendon from becoming visible through the surgical field.
Third, preserve the pretarsal orbicularis muscle along the medial margin. This muscle provides an additional soft-tissue layer over the tendon, and sacrificing it—though sometimes done for crease definition—leaves the tendon bare and visually dominant. In FFS, the trade-off between a sharply defined crease and a padded, smooth contour always favors the latter. A soft, natural crease with volume preservation achieves a more convincing feminine result than a surgically crisp crease with a hollowed, skeletal medial canthus.
Volume Restoration: Micro-Fat Grafting for the Hollowed Periorbital Region
Despite meticulous conservative technique, some patients—particularly those with prior over-resected blepharoplasty—present with established periorbital hollowing that demands volume restoration. Micro-fat grafting has emerged as the gold standard for this challenge, offering permanent or near-permanent volume replacement with the patient’s own tissue.
The micro-fat grafting technique for the upper medial canthus differs from body contouring fat transfer in several critical ways. First, harvest fat from the inner thigh or abdomen using a 2-mm cannula with low negative pressure—manual syringe aspiration, not machine liposuction. The low-pressure technique preserves adipocyte viability and reduces the proportion of ruptured cells in the graft. Second, process the harvested fat through a closed-system filter to remove oil and blood, leaving concentrated, viable fat parcels.
Third, inject the processed fat in micro-quantities—0.05–0.1 cc per pass—using a 0.7-mm blunt cannula. Layer the fat in the sub-orbicularis plane above the medial canthal tendon, building volume incrementally rather than depositing a single bolus. Overcorrection by approximately 30% accounts for the predictable resorption rate, though experienced surgeons can calibrate this based on individual tissue characteristics. Avoid intramuscular injection near the superior oblique, as this can cause restrictive strabismus.
For patients requiring finer contour adjustments and skin quality improvement, nanofat injection offers an elegant complement. Nanofat—mechanically emulsified fat processed to a liquid consistency—contains adipose-derived stem cells and growth factors that improve skin texture, reduce pigmentation, and provide subtle volumization in the superficial periorbital layers. Used in combination with structural micro-fat, nanofat addresses both the volume deficit and the overlying skin quality, delivering results that filler-based treatments cannot replicate.
The Forehead-Blepharoplasty Relationship: Why Isolated Upper Lid Surgery Often Falls Short
Upper eyelid contour in trans women cannot be evaluated in isolation from the forehead and brow. The masculine supraorbital ridge projects anteriorly and inferiorly, casting a shadow over the upper lid that exaggerates the appearance of fat herniation. When a surgeon performs blepharoplasty FFS without addressing the brow bossing, the optical illusion of excess upper lid fat persists postoperatively—even after fat has been adequately conservatively reduced. This drives the surgeon to remove more fat than necessary, setting the stage for the skeletal eye deformity once swelling subsides.
The correct sequence is to address the forehead first. Type III forehead contouring—burring the anterior table of the frontal sinus, setback of the supraorbital rim, and reconstruction with titanium mesh or bone paste—reduces the overhanging shadow and changes the perceived volume of the upper lid. After forehead contouring, what appeared to be a bulky fat pad often reveals itself as a normal amount of tissue obscured by bony shadowing. The blepharoplasty can then proceed with genuine conservation rather than chasing an optical illusion.
This integrated approach—forehead contouring followed by conservative blepharoplasty—produces results that isolated lid surgery can never achieve. The A-frame deformity risk drops to near zero because the surgeon is no longer coerced into over-resecting to compensate for an unaddressed bony protrusion. Furthermore, the combined approach produces a harmonious brow-to-lid transition that reads as naturally feminine, whereas blepharoplasty alone often results in a feminized lid beneath a masculine brow—an aesthetic mismatch that defeats the purpose of the surgery.
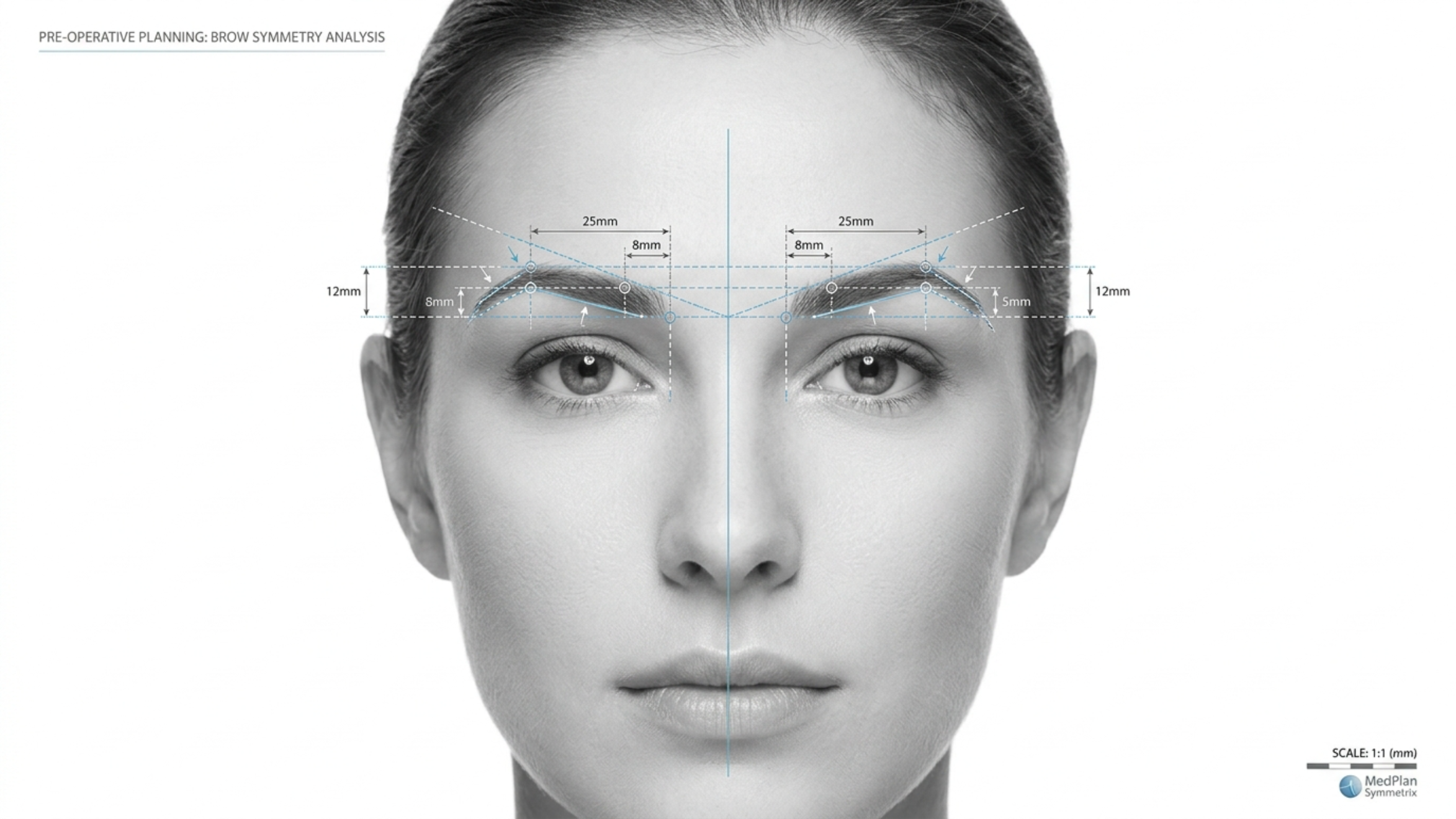
Patient Selection and Preoperative Planning for Feminine Periorbital Results
Not every trans woman requires upper-lid blepharoplasty during FFS. In fact, unnecessary blepharoplasty in patients with adequate fat volumes risks introducing a deformity where none existed. Preoperative planning must distinguish between genuine fat excess and pseudoherniation caused by brow ptosis or forehead prominence.
The assessment begins with the patient in an upright position, brows relaxed. If the brow rests at or above the superior orbital rim and the lid appears full, genuine fat excess may be present. If the brow sags below the rim, the apparent lid fullness may represent brow fat displaced inferiorly—a scenario where brow repositioning alone solves the problem without touching the lid fat. Next, assess the depth of the superior sulcus by palpating the lid just below the brow. A deep, hollow sulcus suggests fat atrophy; blepharoplasty in this context risks catastrophic hollowing.
Document the medial canthal angle from multiple angles—frontal, three-quarter, and close-up. Photograph the medial canthus with side lighting to accentuate any early A-frame tendency. Patients with a naturally shallow medial canthal angle and thin skin are at highest risk for postoperative tendon exposure; for these individuals, a non-excisional approach using skin-only removal with fat preservation may be the safest path. Finally, review the duration and consistency of hormone therapy. Patients on long-term estrogen tend to have better periorbital fat distribution, while those with shorter treatment durations may retain more masculine fat patterns—and should be approached with even greater conservation.
Step-by-Step Clinical Guide: Avoiding the Skeletal Eye Deformity
Translating preservation principles into consistent clinical outcomes demands a disciplined, step-by-step protocol. The following seven-step guide applies to every primary and revision transgender blepharoplasty case.
- Assess the brow-lid relationship before marking the lid. Determine whether brow repositioning or forehead contouring will reduce apparent lid fullness, eliminating the need for fat excision entirely.
- Mark the incision conservatively with the patient upright. Set the medial extent 4 mm lateral to the canthal angle. Identify the vascular arcade as the medial boundary for fat excision.
- Open the central septum and deliver the A2 fat pad. Resect only the prolapsing dome—never the deep component. Allow the residual fat to retract spontaneously without manipulation.
- Open the medial septum with a pinpoint incision. Identify the A1 fat pad by its color and texture. Excise strictly the protruding dome, preserving at least 70% of the total pad volume.
- Cauterize meticulously with bipolar forceps. Confirm hemostasis with repeated irrigation and inspection. Even minor bleeding in this compartment risks retrobulbar hematoma.
- Close the septum loosely or leave it open to allow natural fat redraping. Do not suture the septum tightly—this can create an unnatural adhesion between fat and skin, producing contour irregularities.
- Plan for micro-fat grafting in revision cases where the medial canthal tendon is already visible. Inject in micro-layers using a 0.7-mm cannula, overcorrecting by 30% to accommodate predictable resorption.
Each step in this protocol reinforces the overriding principle: preserve more than you remove. The surgeon who operates with restraint produces results that endure; the surgeon who operates with conventional aggressiveness produces results that mandate revision. The choice is not between a defined crease and a full lid—you can have both if you respect the anatomy. Ready to discuss your periorbital feminization plan with a surgeon who prioritizes preservation? Apply now to schedule your personalized consultation.
Long-Term Volumetric Changes: What Happens to Preserved Fat Over Time
A common concern among patients and surgeons alike is whether preserved periorbital fat will maintain its volume long-term or gradually atrophy. The evidence, reinforced by clinical experience, shows that conservatively treated upper eyelid surgery fat volumes remain remarkably stable when the deep fat is left undisturbed and its blood supply is preserved.
Unlike grafted fat—which undergoes unpredictable resorption rates of 30–60% depending on technique—native fat that has never been manipulated retains its vascular pedicle and cellular architecture. The 70% of the A1 pad left in situ during preservation blepharoplasty continues to function as living tissue, responding to hormonal signals and aging changes just as it would in an unoperated lid. This is the fundamental advantage of preservation over excision followed by grafting: native tissue outperforms any replacement in the long term.
That said, the aging process affects all periorbital tissue. Over decades, some volume loss is inevitable regardless of surgical technique. The critical difference is that preservation-based patients begin their postoperative course with a substantial volumetric reserve. When age-related atrophy occurs in a patient who retained 70% of her A1 fat, she still has enough volume to maintain a feminine contour. When the same process occurs in a patient whose A1 pad was completely excised, she has zero reserve—and the skeletal eye deformity appears or worsens precipitously. Planning for decades, not months, is the essence of ethical and effective upper eyelid contouring in FFS.
When Revision Is Necessary: Secondary Correction of the Skeletal Eye
Despite best efforts, some patients present with established skeletal eye deformity from prior surgery. Revision blepharoplasty in this context is one of the most technically demanding procedures in periorbital surgery. The tissues are scarred, the fat planes are obliterated, and the medial canthal tendon may be densely adherent to the overlying skin. Success demands meticulous scar release, careful fat grafting, and realistic patient expectations.
The revision surgical sequence begins with complete release of the skin-medial canthal tendon adhesions. This requires subcutaneous dissection in a plane superficial to the tendon, gently separating the skin from the underlying scar without disrupting the tendon itself. Once freed, the skin can redrape naturally over the grafted fat rather than being tethered to the tendon. Following adhesion release, micro-fat grafting is performed as described earlier, depositing 0.5–1.0 cc of processed fat in multiple sub-orbicularis passes. The endpoint is gentle overcorrection—with the understanding that final contour stability will not be assessable for 6–12 months postoperatively.
For patients with severe tissue deficit or poor graft take, staged grafting sessions may be necessary. A minimum interval of six months between stages allows the grafted fat to establish its blood supply and allows the surgeon to assess which areas have retained volume and which require supplemental treatment. Nanofat injections at the second stage can refine skin quality in the medial canthal region, reducing translucency that makes the underlying structures more visible. Patience is the defining virtue in revision periorbital hollowing correction—rushing to achieve the final result in a single stage often produces suboptimal contour and the need for yet another revision.

The Chip Meridian Theory: Understanding Fat Zones in the Upper Eyelid
A useful conceptual framework for preservation-based blepharoplasty in FFS divides the upper eyelid fat into three functional zones: the central zone (A2), the transition zone, and the protected medial zone (A1). Each zone has a distinct safe excision threshold, and understanding these thresholds prevents the skeletal eye deformity from occurring in the first place.
The Central Zone (A2) permits moderate excision—up to 50% of the prolapsing volume can be safely removed because this fat pad is large, well-vascularized, and not adjacent to visible tendons or critical muscles. Even when some resorption occurs postoperatively, the central zone has sufficient structural reserve to maintain lid contour.
The Transition Zone—the area where the central and medial fat pads meet—requires caution. Excision here should be limited to the obviously prolapsing fat dome, with the deeper layers left intact. The transition zone is the anatomical watershed where A-frame deformity begins; aggressive excision in this region creates the angular hollow at the apex of the A-frame.
The Protected Medial Zone (A1) is the surgical equivalent of a restricted area. Excision must not exceed 30% of the total pad volume, and the deep portion of the pad must remain absolutely untouched. This zone surrounds the medial canthal tendon and the trochlea—structures whose exposure or irritation defines the skeletal eye. Respecting these three zones turns preservation from a philosophy into a concrete, intraoperative decision-making protocol that any trained surgeon can follow.
Beyond the Upper Lid: Creating Feminine Harmony Across the Periorbital Region
The skeletal eye deformity rarely exists in isolation. When upper-lid fat is over-resected, the entire periorbital region loses cohesion. The brow appears heavier by contrast, the lower lid fat pads appear relatively prominent, and the midface seems disconnected from the upper face. Addressing the feminine eye surgery outcome requires consideration of all periorbital elements, not just the upper lid.
Temporal lifting via endoscopic temporal lift repositions the lateral brow, reducing the weight of tissue bearing down on the upper lid and decreasing the apparent need for fat excision. Cheek augmentation restores midface volume, creating a smooth transition from the lower lid to the cheek that draws the eye downward and away from any residual upper lid hollowing where it exists. When these procedures are combined with conservative upper-lid blepharoplasty, the result is periorbital harmony—a region where each element supports and enhances the others rather than competing for attention.
The take-home message for patients and surgeons is straightforward: the feminine eye is not created by removal. It is created by preservation, repositioning, and strategic augmentation. Aggressive fat excision produces a lid that looks operated, hollowed, and older than the patient’s chronological age—none of which serve the goal of gender-affirming transformation. Blepharoplasty in FFS, when executed with preservation principles, delivers results that are both beautiful and enduring, allowing the patient’s true identity to shine through eyes that.

Frequently Asked Questions
What is the skeletal eye deformity in FFS blepharoplasty?
The skeletal eye deformity occurs when over-resection of upper eyelid fat exposes the medial canthal tendon and periorbital bone, creating a hollowed, angular appearance that masculinizes rather than feminizes the eye. It typically results from aggressive A1 fat pad removal.
How much of the A1 fat pad should be preserved during blepharoplasty in FFS?
At least 70% of the A1 fat pad should remain in situ. Only the visibly prolapsing dome should be excised, while the deep portion cushioning the medial canthal tendon and superior oblique trochlea must stay undisturbed.
Why does conventional blepharoplasty fail in trans women?
Conventional blepharoplasty aims for a crisp, hollowed lid crease appropriate for cisgender women with naturally full periorbital regions. Trans women have prominent brow bones that amplify post-fat-removal hollowing, making the same approach produce a masculinizing skeletal appearance.
Can the skeletal eye deformity be corrected after surgery?
Yes, revision with micro-fat grafting can restore volume, but the procedure is technically demanding due to scarred tissue planes. Staged grafting sessions with six-month intervals between procedures achieve the best long-term results.
What is the A-frame deformity and how does it relate to the medial canthal tendon?
The A-frame deformity is an angular, tent-shaped hollow at the medial canthus caused by complete A1 fat excision that exposes the medial canthal tendon beneath thin skin. It is the most recognizable sign of over-resected upper eyelid blepharoplasty.
Should forehead contouring be performed before blepharoplasty in FFS?
Yes, forehead contouring should precede blepharoplasty because reducing the supraorbital ridge eliminates the bony shadow that makes the upper lid appear overfull. This allows a truly conservative fat-preserving approach to blepharoplasty.
How does hormone replacement therapy affect blepharoplasty planning?
Long-term estrogen therapy redistributes periorbital fat toward a feminine pattern, while shorter durations retain more masculine fat distribution. Patients with shorter treatment histories require even more conservative fat removal to avoid long-term hollowing.