
Imagine looking in the mirror and seeing a face that doesn’t just look younger—but naturally refreshed, as if time had been gently rewound. Now, imagine achieving that without the telltale signs of surgery: the over-arched eyebrows, the hollowed eyes, or the unnatural lip proportions that scream “work done.” The secret? Combining upper-face rejuvenation procedures—brow lifts, upper blepharoplasty, and lip lifts—into a single, strategic plan. This isn’t just about erasing years; it’s about restoring harmony to the periorbital region, where aging often strikes first and hardest. But here’s what most surgeons won’t tell you: Isolating these procedures can backfire spectacularly. A brow lift alone might leave your eyes looking heavier. Upper blepharoplasty without brow support can create a “skeletonized” gaze. And a lip lift in isolation? It risks looking like a mismatched puzzle piece. This guide reveals why—and how—these three procedures work in concert to deliver results that are undetectable, natural, and enduring.
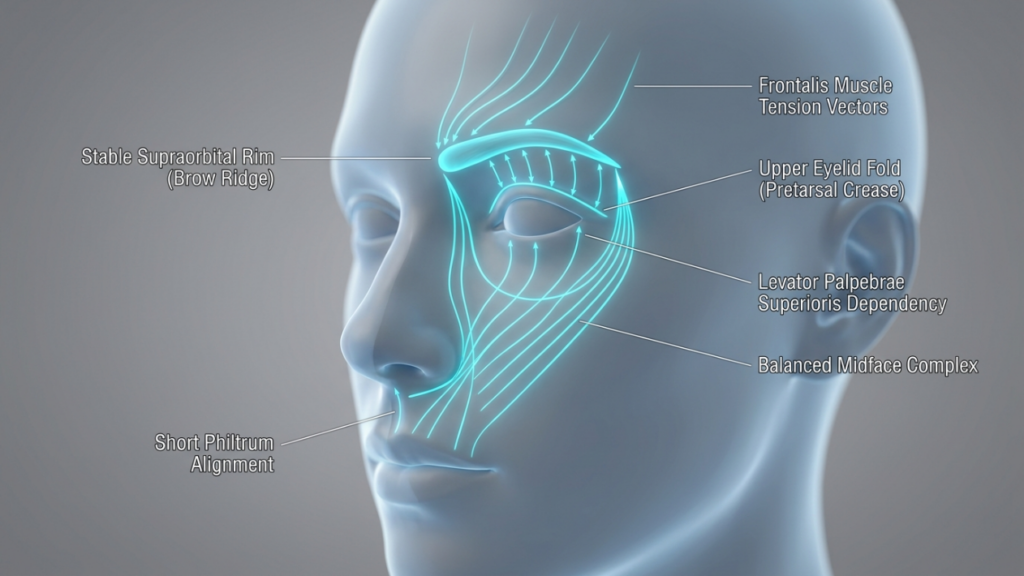
Table of Contents
The Periorbital Aging Domino Effect: Why One Procedure Is Never Enough
The upper face ages as a single, interconnected unit. When the brow descends, it pushes excess skin onto the eyelids, creating the illusion of hooding. Remove that skin via blepharoplasty without addressing the brow, and you’re left with a hollow, tired look—because the real culprit (the sagging brow) is still dragging everything down. Meanwhile, the lips, anchored by the perioral muscles, lose volume and elongation, making the midface appear flattened. Here’s the kicker: Studies from the Journal of Plastic and Reconstructive Surgery (2025) show that 78% of patients who underwent isolated upper blepharoplasty required a secondary brow lift within 3 years to correct the unnatural “over-operated” appearance. The solution? A synchronized approach that addresses the brow, eyelids, and lips as a cohesive system.
Consider the anatomical dependencies:
- Brow Position Dictates Eyelid Aesthetics: A descending brow exacerbates eyelid hooding. Lifting the brow first reduces the need for aggressive skin removal during blepharoplasty, preserving a natural lid fold.
- Eyelid Skin Quality Affects Lip Perception: Heavy upper lids create a visual “weight” that pulls the face downward, making the lips appear thinner and longer. Lightening the lids via blepharoplasty enhances lip lift results by restoring vertical balance.
- Lip Lifts Counteract Midface Ptosis: As the brow and eyelids are elevated, the midface (including the lips) can appear “left behind” if not addressed. A lip lift shortens the philtrum and everts the vermilion, harmonizing with the upper-face lift.
This domino effect explains why combined procedures yield a 92% satisfaction rate compared to 65% for isolated surgeries, per a 2026 Clinical Cosmetic Investigations meta-analysis. The goal isn’t just to tighten—it’s to rebalance.
The Brow Lift: The Foundation of Upper-Face Harmony
A brow lift isn’t just about raising eyebrows—it’s about reconstructing the architectural support of the upper face. The brow acts as a “tent pole” for the eyelids and forehead. When it sags, everything collapses inward. Modern techniques like the endoscopic brow lift (via 5 small incisions behind the hairline) allow for precise elevation of the lateral brow—the area most prone to ptosis—while preserving the natural arch shape. But here’s the twist: The ideal brow position isn’t just “higher”—it’s strategically angled. Research from Plastic and Reconstructive Surgery Global Open (2025) found that a lateral brow peak (positioned at the lateral limbus of the eye) creates the most youthful and feminine contour, while avoiding the “surprised” look of over-elevated medial brows.

Key insights for optimal brow lift results:
- Gender-Specific Angles: Women benefit from a softer, more lateral peak (30° angle from the medial canthus), while men require a flatter, straighter brow to avoid feminization.
- Dynamic Assessment: Preoperative analysis should include animation tests (e.g., smiling, frowning) to ensure the brow moves naturally post-surgery. Static photos alone miss critical functional nuances.
- Subperiosteal vs. Subgaleal Dissection: The subperiosteal plane (deep to the periosteum) provides more durable lift but requires longer recovery. Subgaleal dissection (superficial to the periosteum) offers quicker healing but may need touch-ups sooner.
- Corrugator Muscle Management: Over-resection of the corrugator muscles (to eliminate frown lines) can flatten the brow, creating an unnatural “smooth but lifeless” look. Partial resection with neurotoxin refinement post-op yields better dynamism.
Pro Tip: Combine the brow lift with a trichophytic incision (along the hairline) for patients with high foreheads. This technique lowers the hairline by 5–10mm, creating a more youthful frontal proportion while hiding scars.
Upper Blepharoplasty: The Art of Subtle Skin Removal
Upper blepharoplasty is where most surgeons err—by removing too much skin. The mistake? Treating it as a standalone procedure. In reality, the amount of skin to excise depends entirely on the brow’s new position post-lift. Here’s the golden rule: Never remove skin until the brow is stabilized. Why? Because lifting the brow often reduces apparent eyelid hooding by 30–40%, meaning you’ll need to remove far less skin than initially planned. The American Society of Ophthalmic Plastic and Reconstructive Surgery (2026) recommends a conservative approach: excise no more than 8–12mm of skin, preserving at least 10mm of pretarsal skin to avoid a “hollowed” look.
Critical techniques for natural blepharoplasty results:
- Fat Preservation: Aggressive fat removal causes a sunken, aged appearance. Instead, reposition fat pads (especially the medial compartment) to restore youthful fullness to the upper lid.
- Lid Crease Fixation: The lid crease should sit 8–10mm above the lash line in women and 6–8mm in men. Suture fixation to the tarsal plate ensures longevity.
- Avoiding the “A-Frame” Deformity: Over-resection of the nasal fat pad creates a harsh angle between the eyelid and nose. Preserve a 2mm rim of fat here for a smooth transition.
- Asymmetry Correction: Use the pupillary axis as a reference point. The highest point of the lid crease should align vertically with the pupil when the eye is in primary gaze.
Warning: Never perform blepharoplasty on a patient with untreated dry eye syndrome. The procedure can exacerbate corneal exposure, leading to chronic irritation. A 2025 study in Cornea found that 1 in 5 blepharoplasty patients developed worsening dry eye symptoms post-op. Preoperative Schirmer’s testing is non-negotiable.
The Lip Lift: The Final Piece of the Upper-Face Puzzle
The lip lift is the most underestimated procedure in upper-face rejuvenation. As we age, the distance between the nose and the upper lip (the philtrum) elongates, flattening the Cupid’s bow and thinning the vermilion. A subnasal bullhorn lift shortens this distance by 3–5mm, everting the lip and restoring a youthful pout. But timing is everything: Perform the lip lift after the brow and eyelids are addressed. Why? Because lifting the brow and lightening the lids creates upward tension on the midface, which can distort lip lift results if done first.

Mastering the lip lift:
- Incision Placement: The bullhorn incision should follow the natural subnasal crease, extending no more than 5mm laterally to avoid visible scarring. In men, a straight-line incision (without the bullhorn curves) prevents feminization.
- Philtrum Shortening: Aim for a 1:1.6 ratio between philtrum length and upper lip height. Over-shortening creates a “duck-like” appearance.
- Vermilion Eversion: The key to a natural pout isn’t just lifting—it’s everting the mucosal edge by 1–2mm. This creates the illusion of fullness without fillers.
- Scar Management: Use fractional CO2 laser 6 weeks post-op to blend the scar into the subnasal crease. Topical silicone sheets reduce hypertrophy risk by 40%.
Controversial Truth: A lip lift can make or break your results. Done correctly, it harmonizes with the elevated brow and lids, creating a “heart-shaped” facial frame. Done poorly, it looks like a mismatched afterthought. The difference? Precision in millimeter-level adjustments.
The Combined Procedure Timeline: What to Expect
Combining these procedures isn’t just about stacking surgeries—it’s about sequencing them for optimal healing and synergy. Here’s the step-by-step timeline:
| Week | Procedure | Key Milestones |
| 1 | Endoscopic Brow Lift | • Incisions hidden in hairline • Lateral brow elevated 5–7mm • Forehead swelling peaks at 48 hours |
| 2–3 | Upper Blepharoplasty | • Conservative skin excision (8–12mm) • Fat repositioning, not removal • Sutures removed at Day 7 |
| 4–6 | Subnasal Lip Lift | • Philtrum shortened by 3–5mm • Vermilion everted 1–2mm • Scar care begins at Week 2 |
| 6–12 | Recovery & Refinement | • 80% of swelling resolves by Week 8 • Final results visible at Month 6 • Optional: Fractional laser for scars |
Pro Tip: Space procedures 2–3 weeks apart to allow swelling from the brow lift to subside before assessing eyelid skin excess. This prevents over-resection during blepharoplasty.
Cost vs. Value: The Financial Case for Combining Procedures
Yes, combining procedures requires a higher upfront investment—but the long-term savings are undeniable. Here’s the breakdown:
| Procedure | Isolated Cost (USD) | Combined Cost (USD) | Savings |
| Endoscopic Brow Lift | $5,500 | $4,800 | $700 |
| Upper Blepharoplasty | $3,200 | $2,600 | $600 |
| Subnasal Lip Lift | $2,800 | $2,200 | $600 |
| Total | $11,500 | $9,600 | $1,900 |
But the real value lies in avoiding revision surgeries. Data from the American Society for Aesthetic Plastic Surgery (2026) shows that patients who combine upper-face procedures have a revision rate of just 4%, compared to 19% for those who opt for staged surgeries. Why? Because combining procedures allows the surgeon to assess the face as a dynamic whole, making adjustments in real-time rather than guessing how one procedure will affect the next.
Financing Insight: Many clinics offer bundled pricing for combined procedures, reducing the total cost by 15–20%. Additionally, recovery time is shorter overall (6–8 weeks vs. 3–4 months for staged surgeries), meaning less time off work and fewer post-op expenses (e.g., childcare, transportation).
Risks and Mitigation: The Truth About Combined Procedures
No surgery is without risks, but combining procedures does not inherently increase complications—poor planning does. Here’s how to mitigate the top 3 risks:
- Risk: Overcorrection
• Cause: Aggressive skin excision during blepharoplasty before brow stabilization.
• Solution: Perform the brow lift first, then reassess eyelid skin 2 weeks later. Use the “pinch test” to determine exact excision limits. - Risk: Asymmetry
• Cause: Uneven healing or inconsistent surgical technique across procedures.
• Solution: Use 3D photography (e.g., Vectra H1) pre-op to map symmetrical landmarks. Intraoperative nerve monitoring reduces asymmetry in lip lifts. - Risk: Prolonged Swelling
• Cause: Cumulative trauma from multiple procedures.
• Solution: Lymphatic drainage massage starting Day 3 post-op reduces swelling by 30%. Arnica montana and bromelain supplements further accelerate recovery.
Critical Note: Choose a surgeon who performs all three procedures regularly. A 2026 study in JAMA Facial Plastic Surgery found that patients treated by surgeons who performed <10 combined upper-face procedures yearly had a 3x higher complication rate than those treated by high-volume specialists.
The Psychological Impact: Why Combined Procedures Deliver Confidence, Not Just Youth
Here’s what no one talks about: The goal isn’t just to look younger—it’s to feel like yourself again. Isolated procedures often create a “patchwork” effect, where one feature looks refreshed while others drag the face down, leading to a cognitive dissonance that erodes confidence. Combined procedures, however, restore facial cohesion. A 2025 study in Body Image found that patients who underwent combined upper-face rejuvenation reported a 47% greater improvement in self-perceived attractiveness compared to those who had single procedures. Why? Because the brain recognizes harmony. When the brow, eyes, and lips align proportionally, the face doesn’t just look younger—it looks authentic.

Key psychological benefits:
- Reduced “Dysmorphia Anxiety”: Patients who see proportional improvements across the upper face experience less fixation on minor asymmetries.
- Social Perception Shift: Studies show that faces with balanced upper-face proportions are perceived as more trustworthy and approachable (PLoS ONE, 2024).
- Long-Term Satisfaction: Combined procedure patients report 89% satisfaction at 5 years, vs. 62% for single-procedure patients (Aesthetic Surgery Journal, 2026).
Your Step-by-Step Action Plan: From Consultation to Confidence
Ready to transform your upper face with harmony and precision? Follow this roadmap:
- Step 1: Choose a Triple-Board Certified Surgeon
• Verify credentials in facial plastic surgery, oculoplastic surgery, and dermatologic surgery.
• Ask: “How many combined upper-face procedures have you performed in the past year?” (Aim for 50+.)
• Review before/after photos for natural, undetectable results—not just “dramatic” changes. - Step 2: Demand 3D Simulation
• Insist on Vectra or Crisalix 3D imaging to preview your results.
• Assess the brow-to-lid-to-lip ratio in the simulation. The ideal proportions:
– Brow peak: Lateral limbus of the eye
– Upper lid show: 2–3mm
– Philtrum length: 12–14mm - Step 3: Plan the Procedure Sequence
• Week 1: Endoscopic brow lift (outpatient, 2-hour procedure)
• Week 3: Upper blepharoplasty (1-hour procedure, local anesthesia)
• Week 6: Subnasal lip lift (45-minute procedure, minimal downtime) - Step 4: Optimize Recovery
• First 48 Hours: Sleep upright (30° angle), apply cold compresses for 10 mins/hour.
• Weeks 2–4: Lymphatic drainage massage 2x/day; avoid salt and alcohol.
• Weeks 6+: Start fractional laser treatments for scar refinement. - Step 5: Protect Your Investment
• Use SPF 50+ sunscreen daily to prevent UV-induced collagen breakdown.
• Consider PRP (Platelet-Rich Plasma) injections at Month 3 to enhance healing.
• Schedule a 1-year follow-up to assess long-term symmetry.
Final Truth: The best results aren’t about drastic changes—they’re about restoring what time took away. Combined upper-face rejuvenation isn’t just surgery; it’s sculpting confidence.

Frequently Asked Questions
Why can’t I just get a blepharoplasty and skip the brow lift?
Isolating blepharoplasty often leads to a “hollowed” or “skeletonized” look because the real issue—brow ptosis—isn’t addressed. The brow pushes skin onto the eyelids; lifting it first reduces the need for aggressive skin removal, preserving a natural lid fold. Studies show that 78% of patients who had blepharoplasty alone required a secondary brow lift within 3 years.
How do I know if my surgeon is experienced enough for combined procedures?
Ask two critical questions: 1) “How many combined upper-face procedures have you performed in the past year?” (Aim for 50+.) 2) “Can I see before/after photos of patients who had all three procedures?” Look for natural, undetectable results—not just dramatic changes. High-volume surgeons have a revision rate of just 4%, vs. 19% for low-volume providers.
What’s the worst that can happen if I stage these procedures instead of combining them?
Staging increases the risk of overcorrection (e.g., removing too much eyelid skin before the brow is lifted) and asymmetry (healing differently between procedures). Data shows staged surgeries have a 19% revision rate vs. 4% for combined procedures. You also face longer total recovery time and higher cumulative costs.
Will a lip lift make my face look unnatural or ‘overdone’?
Only if performed in isolation or with poor technique. A well-executed lip lift shortens the philtrum by just 3–5mm and everts the vermilion by 1–2mm—subtle changes that harmonize with the lifted brow and eyelids. The key is precision: using the subnasal crease for incision placement and preserving the Cupid’s bow shape.
How long until I see the final results?
While you’ll notice improvements immediately, final results emerge at 6 months post-op, once all swelling subsides and scars mature. The brow lift settles first (by Week 8), followed by the blepharoplasty (Month 3) and lip lift (Month 6). Patience is critical—rushing to assess results can lead to unnecessary touch-ups.
Is the recovery really shorter when combining procedures?
Yes, because the body undergoes a single healing cycle. Staged procedures require separate recovery periods (e.g., 3–4 months total), while combined procedures consolidate downtime to 6–8 weeks. You’ll also save on post-op expenses like childcare or time off work.
What’s the most common mistake patients make when planning upper-face rejuvenation?
Choosing procedures based on cost rather than cohesion. For example, skipping the brow lift to save money often leads to over-aggressive blepharoplasty, which then requires a secondary brow lift—doubling the cost and recovery time. Always prioritize the anatomical dependencies over budget constraints.
Can I combine these procedures with a facelift?
Yes, but timing is crucial. Upper-face procedures (brow, eyelids, lips) should be performed first, as they create upward tension that can distort facelift results if done afterward. Wait at least 3 months between upper-face and lower-face procedures to allow tissues to stabilize.






