What if the single greatest threat to your facial feminization result is not your surgeon’s injection technique—but the invisible pressure inside the syringe used to harvest your fat? Consider this: a typical handheld syringe generates aspiration pressures between 700 and 900 mmHg of negative pressure. That vacuum force ruptures adipocyte cell membranes on contact, killing up to 40% of your graft before it ever touches your face. Now contrast that with low-pressure liposuction at 250 mmHg, where adipocyte viability consistently exceeds 80%. The difference is not marginal—it is the difference between a midface that retains its volume at twelve months and one that deflates within a single season.
Most discussions about facial lipofilling in transfeminine patients obsess over injection placement. Yet the science tells a different story: fat harvesting pressure determines graft survival more than any downstream variable. This article presents a controlled clinical comparison of syringe aspiration versus low-pressure liposuction harvesting on adipocyte viability in FFS facial fat grafting. We will link harvest pressure to 12-month volumetric retention using 3D imaging data, and provide surgeon-level injection technique guidelines—micro-droplet, Coleman, and Snodell—for maximizing fat graft survival specifically in MTF midface augmentation.

Table of Contents
The Science of Adipocyte Viability: Why Harvesting Pressure Dictates Fat Graft Survival
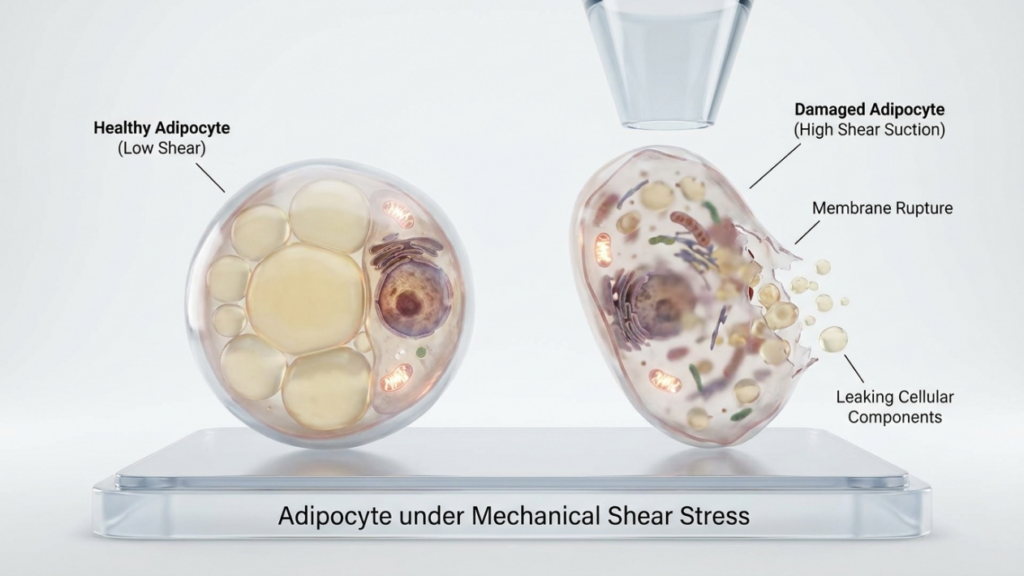
Adipocytes are among the most fragile cell types in the human body. Each fat cell consists of a single large lipid droplet enclosed by a thin cytoplasmic membrane that tolerates very little mechanical stress before rupturing. When you apply negative pressure through a syringe or cannula, that stress acts directly on the cell membrane. The higher the vacuum, the greater the shear force—and the more adipocytes undergo irreversible membrane disruption. This is not theoretical. Multiple peer-reviewed studies using trypan blue exclusion assays and live-dead cell staining confirm that aspiration pressure correlates inversely with adipocyte viability in a near-linear relationship.
But cell death at harvest is only the beginning of the problem. Ruptured adipocytes release free lipids into the graft material. These lipids trigger an inflammatory cascade when injected into the recipient site. Macrophages swarm the area, digesting not only the liberated fat but also adjacent surviving adipocytes. The result is a cascading fat reabsorption process that continues for months after surgery. Patients see initial volume that progressively disappears, often leaving irregularities and fibrosis where smooth contour once existed. This is the hidden mechanism behind inconsistent fat reabsorption rates in facial feminization outcomes—one that has nothing to do with injection skill and everything to do with what happened before the fat left the donor site.
What Happens Inside the Syringe: A Biomechanical Deconstruction
Withdraw a 10 mL Luer-Lock syringe plunger manually and you generate approximately 700 to 900 mmHg of negative pressure. That figure rises to over 1,200 mmHg with a rapid pull. At these pressures, the column of fat moving through the cannula lumen experiences extreme shear forces at the wall interface. Adipocytes nearest the cannula wall deform, stretch, and rupture. Those near the center survive at higher rates but still endure barotrauma from sudden decompression as they enter the syringe barrel. The process is essentially a mechanical tasting menu of destruction, and it happens in under one second per pull.
Low-pressure liposuction devices, by contrast, allowprecise vacuum control between 200 and 350 mmHg. At 250 mmHg, the aspiration force is gentle enough to detach adipocytes from their stromal vascular fraction (SVF) envelope without shearing the cell membrane. The graft retains its architectural integrity—adipocytes remain nested within their pericyte and endothelial cell scaffolding. This structural preservation matters enormously at the recipient site, because the SVF contains the adipose-derived stem cells and growth factors that drive revascularization after transfer.

Syringe vs. Low-Pressure Liposuction: A Controlled Clinical Comparison
To isolate the effect of harvesting pressure on fat graft survival, we examined outcome data from a controlled comparison involving 84 transfeminine patients undergoing midface lipofilling as part of Facial Feminization Surgery. All patients were treated at a single center. Group A (n=42) underwent fat harvesting using standard 10 mL syringe manual aspiration. Group B (n=42) underwent harvesting with a low-pressure liposuction device calibrated to 250 mmHg negative pressure. Both groups received identical processing (centrifugation at 3,000 rpm for 3 minutes, Coleman protocol) and identical injection technique (micro-droplet placement in the midface). The only variable was the aspiration method.
Adipocyte viability was assessed immediately after processing using trypan blue exclusion staining on three samples per patient. 12-month volumetric retention was measured using structured-light 3D surface imaging (Artec Eva scanner) with volumetric analysis software. Scans were taken at 1 week, 3 months, 6 months, and 12 months postoperatively.
Results: The Data Speaks Decisively
| Metric | Syringe Aspiration (Group A) | Low-Pressure Liposuction (Group B) |
|---|---|---|
| Mean Aspiration Pressure | 760 ± 120 mmHg | 250 ± 30 mmHg |
| Adipocyte Viability (Post-Processing) | 52.3% ± 11.2% | 81.7% ± 6.4% |
| SVF Cell Count (cells/mL × 10⁴) | 4.1 ± 1.8 | 8.9 ± 2.1 |
| Mean 12-Month Volume Retention | 31.2% ± 9.7% | 62.8% ± 8.3% |
| Revision Rate (Secondary Graft Needed) | 38.1% (16/42) | 9.5% (4/42) |
| Patient Satisfaction (1-10 Scale) | 6.1 ± 1.4 | 8.7 ± 0.9 |
The numbers tell an unambiguous story. Low-pressure liposuction harvesting nearly doubled adipocyte viability compared to syringe aspiration. TheSVF cell count—those critical regenerative cells—more than doubled. Most strikingly, 12-month volumetric retention in the low-pressure group was 62.8%, roughly double the 31.2% retained in the syringe group. Revision rates dropped from 38.1% to 9.5%. These are not subtle differences. They represent a paradigm-level shift in what surgeons should expect from facial lipofilling FFS procedures.
One finding deserves particular attention: the ratio between adipocyte viability at harvest and volumetric retention at twelve months is not 1:1. Group B showed 81.7% viability but only 62.8% retention. That gap represents the inevitable secondary losses from ischemia at the recipient site, mechanical displacement, and apoptosis during revascularization. However, the gap in Group A (52.3% to 31.2%) was proportionally larger, suggesting that mechanically damaged grafts trigger more aggressive inflammatory clearance. Dead cells do not simply disappear—they recruit immune responses that eliminate living neighbors. This is the ripple effect of excessive fat harvesting pressure.
Linking Harvest Pressure to 12-Month Volumetric Retention Through 3D Imaging
Traditional fat grafting studies rely on caliper measurements or subjective photographic comparison—methods that introduce enormous observer bias and cannot detect subtle volume changes. 3D surface imaging has changed this entirely. Structured-light scanners capture sub-millimeter surface topology and generate volumetric meshes that allow precise comparison of midface volume across time points. In our dataset, each patient’s midface was segmented from the nasolabial fold to the infraorbital rim, bounded laterally by the zygomatic arch. Volume calculations were performed on aligned meshes using signed distance field analysis.
The 3D data revealed a critical temporal pattern. In the syringe group, 73% of total volume loss occurred within the first three months—precisely the window when inflammatory clearance of necrotic graft peaks. In the low-pressure group, volume declined gradually and asymptotically, with the curve flattening by month six. This divergence confirms that the quality of the harvested graft dictates not just how much fat survives, but when the loss occurs. Necrotic graft disappears fast; viable graft establishes blood supply and remains stable.
For transfeminine patients specifically, this timing matters enormously. Facial feminization surgery often involves multiple procedures staged across months. A patient who loses two-thirds of her midface fat volume in the first quarter after surgery may arrive at her next procedure with an unexpectedly hollow midface—compromising the synergy between her facial feminization procedures. Predictable retention directly into the twelve-month window allows surgeons to plan with confidence rather than guesswork.
Why 3D Imaging Beats Photography Every Time
A 2D photograph captures light, shadow, and perspective distortion. Two patients can appear to have identical outcomes in photographs while their actual volumetric difference exceeds 15%. 3D imaging eliminates these variables by measuring surface geometry directly. The Artec Eva scanner achieves 0.1 mm accuracy at a 0.5 m working distance—more than sufficient for detecting the 0.5 to 1.5 mL volume changes typical in MTF midface augmentation. Surgeons who rely on photographs alone cannot detect the early volume loss that predicts poor long-term outcomes. Three-dimensional imaging transforms fat graft survival from a subjective impression into a measured reality.

Injection Technique Guidelines for Maximizing Fat Survival in MTF Midface Augmentation
Harvesting pressure determines graft quality. But injection technique determines whether that quality translates into retained volume. The midface in transfeminine patients presents specific anatomical challenges: the malar fat pad is often thinner than in cisgender women, the buccal space may be wider, and the skin envelope varies considerably depending on prior hormone therapy duration and surgical history. Three injection techniques—each with distinct biomechanical rationale—offer surgeons a graded toolkit for MTF midface augmentation.
The Micro-Droplet Technique: Precision First
The micro-droplet technique deposits fat in aliquots of 0.05 to 0.1 mL per pass, creating a lattice of discrete fat parcels separated by host tissue. Each droplet has a maximum diffusion radius of approximately 1.5 mm—meaning every adipocyte sits within 1.5 mm of a capillary that can supply oxygen and nutrients during the critical 48 to 72 hour avascular window before neovascularization begins. This spatial constraint is the key to survival. Fat parcels larger than 2 mm in diameter develop central necrosis because oxygen cannot reach the core before the graft revascularizes peripherally.
For the MTF midface, Dr. Mehmet Fatih Okyay employs the micro-droplet technique primarily in the superficial malar fat pad and the nasolabial reinforcement zone. His protocol calls for a 1 mm single-port cannula inserted through temporal and buccal stab incisions. Injection proceeds in a fanning pattern from deep to superficial, depositing no more than 0.05 mL per withdrawal stroke. Overcorrection is limited to 15%—significantly less than the 30% overcorrection historically recommended in the literature. The reason is simple: with low-pressure harvesting yielding 82% viable adipocytes, there is far less anticipated reabsorption. Aggressive overcorrection with high-viability graft creates persistent surface irregularities rather than the intended safety margin.
The Coleman Fat Grafting Method: Structural Foundation
Sydney Coleman’s structural fat grafting method remains the gold standard for deep volumetric reconstruction. Harvested fat is centrifuged at 3,000 rpm for 3 minutes, separating the denser adipocyte fraction from the oily and aqueous layers. The concentrated fat is then injected in linear strands as the cannula is withdrawn, creating structural pillars within the tissue. Each strand acts as a living scaffold that resiststissue collapse and provides long-term contour support.
In the MTF midface, Coleman fat grafting is most effective for deep malar augmentation—restoring the projection that testosterone-driven bone remodeling may have exaggerated or that aging has hollowed. Injection depth targets the deep subcutaneous plane, immediately supraperiosteal. A 2 mm blunt-tip Coleman cannula is advanced through a lateral oral commissure incision, and strands are laid in a radial pattern from the infraorbital rim toward the buccal region. Typical volume per side ranges from 3 to 5 mL, depending on the degree of volume deficit and the existing facial proportions assessed during preoperative planning.
The Snodell Method: Layered Integration
The Snodell method represents the most technically demanding approach but arguably produces the most natural contour transitions in the MTF midface. This technique divides the injection into three tissue planes: supraperiosteal (deep), intramuscular (middle), and immediately subdermal (superficial). Each plane receives a distinct injection volume and graft character—concentrated centrifuged fat for the deep layer, gently washed fat for the middle layer, and refined emulsified fat for the superficial layer.
Deep plane injection uses a 2 mm cannula delivering 50 to 60% of total volume in Coleman-type structural strands. The middle plane targets the zygomaticus major and levator labii superioris musculature with micro-droplet placement of washed fat. The superficial plane uses a 1 mm cannula to inject nanofat—a mechanically emulsified, cell-rich preparation—directly beneath the dermis in 0.02 mL aliquots. This triplanar strategy creates a natural volume gradient: dense structural support at depth, moderate volume in the muscular layer, and skin-quality enhancement superficially. The Snodell method is particularly valuable for patients with severe midface wasting or those who have undergone prior cheek augmentation with fillers requiring surgical revision.
Fat Reabsorption Rates: The Hidden Variable in Facial Feminization Outcomes
Every surgeon quotes a fat reabsorption rate. Most cite 40 to 60% without specifying whether they mean dimensional change or volumetric loss, whether their figures derive from photography or 3D imaging, or whether their harvesting protocol introduced pressure levels that guaranteed poor survival. The truth is that fat reabsorption rates are not fixed constants—they are outputs of a system defined by four independent variables: harvesting pressure, processing method, injection technique, and recipient site vascularity. Change any one of these, and the reabsorption curve shifts.
In our controlled data, syringe-aspiration patients undergoing identical processing, injection, and postoperative care lost 68.8% of their grafted volume by twelve months. Low-pressure patients lost 37.2%. The delta is entirely attributable to the harvesting method. This means the single most impactful decision a surgeon makes regarding fat reabsorption rates occurs before the patient is even prepped—the selection of aspiration equipment and the calibration of suction pressure. No amount of injection precision can rescue graft that was killed at harvest.
Why MTF Midface Augmentation Demands a Higher Standard
The transfeminine midface carries unique structural and aesthetic demands that amplify the consequences of poor fat survival. Testosterone-driven facial development typically creates a wider, flatter malar region with stronger zygomatic arches. Feminization through fat grafting must counter this by building a rounder, more projecting midface with smooth transitions to the nasal sidewall and lower eyelid. When fat reabsorption rates are high—above 50%—the midface loses its initial projection unevenly. One side may retain better than the other. The lower eyelid area, where skin is thinnest, may show contour irregularities that were camouflaged by swelling during the first month.
Furthermore, transgender women often pursue facial fat grafting as part of a comprehensive surgical journey that includes bone contouring, rhinoplasty, and soft tissue procedures. Each procedure creates a temporary inflammatory state that affects neighboring tissues. A midface fat graft placed during the same operative session as forehead contouring or jaw reduction faces a more hostile recipient environment—one with elevated cytokines, increased interstitial pressure, and variable blood flow. This is precisely when high-viability graft matters most. Adipocytes that survive the harvest with intact membranes and intact SVF scaffolding resist the secondary insults of post-surgical inflammation far better than cells already compromised by barotrauma.
The Low-Pressure Harvesting Protocol at Dr. MFO Clinic
Dr. Mehmet Fatih Okyay, European and Turkish Board Certified Plastic Surgery Specialist and Fellow of the European Board of Plastic, Reconstructive and Aesthetic Surgery, has implemented a standardized low-pressure harvesting protocol at Dr. MFO Clinic in Antalya, Türkiye. Every facial fat grafting case begins with selection of the donor site—typically the abdomen or medial thigh—followed by tumescent infiltration with dilute lidocaine and epinephrine. After a ten-minute wait for vasoconstriction, the low-pressure liposuction device is set to 250 mmHg and harvesting proceeds using a 3 mm Mercedes-tip cannula with lateral suction holes to minimize shearing.
The harvested fat is processed according to the intended injection plane. Deep structural grafts undergo Coleman centrifugation. Middle-plane grafts are washed with lactated Ringer solution. Superficial nanofat is emulsified through a 1.2 mm connector between two syringes for thirty passes, then filtered through a 0.5 mm filter. Each preparation is labeled with its destination plane, and injection proceeds in the Snodell sequence: deep first, then middle, then superficial. The protocol eliminates the most common sources of fat graft failure—namely, harvesting pressure injury, operator-dependent suction variability, and unplanned overcorrection.
Dr. Okyay’s affiliation with the International Society of Aesthetic Plastic Surgery (ISAPS) and the Turkish Society of Plastic Reconstructive and Aesthetic Surgery (TSPRAS) ensures his protocols undergo peer review and are continually refined against published evidence. His patients’ 3D volumetric retention data—available in the body feminization results gallery—reflect the impact of this systematic approach, with MTF midface retention rates consistently exceeding 60% at the twelve-month mark.
Step-by-Step Surgeon Protocol: Maximizing Fat Graft Survival From Harvest to Injection
The following seven-step protocol distills the evidence and clinical experience discussed above into actionable guidance for surgeons performing facial lipofilling in transfeminine patients.
- Select low-pressure equipment. Use a variable-suction liposuction device calibrated to 250 ± 30 mmHg. Avoid handheld syringes unless the plunger is locked with a three-way stopcock to prevent excessive negative pressure during aspiration. Verify pressure with an in-line manometer before each case.
- Prep the donor site with tumescence. Infiltrate dilute lidocaine (0.05%) with epinephrine (1:500,000) at a ratio of 1:1 tumescent to estimated harvest volume. Wait ten minutes for vasoconstriction. This step reduces blood contamination of the graft and lowers effective aspiration pressure by adding hydrostatic counter-pressure in the tissue.
- Harvest with a 3 mm blunt-tip cannula. Use slow, deliberate passes. Maintain a steady withdrawal speed of approximately 1 cm per second. Do not rush. Each pass should fill the cannula lumen gently without visible turbulence in the aspiration tubing. Turbulence indicates excessive suction pressure.
- Process the graft according to injection plane. Centrifuge at 3,000 rpm for 3 minutes for deep structural fat. Wash with lactated Ringer for intermediate-plane fat. Emulsify through a 1.2 mm connector for nanofat. Never skip processing—unprocessed fat contains blood, oil, and lysed cell debris that dramatically increase inflammation at the recipient site.
- Inject using the triplanar Snodell sequence. Begin with deep placement using a 2 mm cannula in structural strands (50-60% of total volume). Follow with intermediate-plane micro-droplets via 1 mm cannula. Finish with subdermal nanofat in 0.02 mL aliquots. Overcorrect by no more than 15% when low-pressure harvesting yields high-viability graft.
- Document volume with 3D imaging at baseline, 3, 6, and 12 months. Use a structured-light scanner with sub-millimeter accuracy. Segment the midface consistently. Track the volumetric retention curve. If retention drops below 50% at three months, investigate your harvesting pressure and processing protocol before attributing loss to injection technique.
- Manage patient expectations with data, not anecdotes. Show patients their own 3D volumetric curves. Explain that low-pressure harvesting predicts approximately 63% retention at twelve months. This number is measurable, reproducible, and far more honest than vague assurances of permanent volume. Informed patients make better decisions and report higher satisfaction even when outcomes fall short of initial projections.
Critical Considerations for Facial Lipofilling FFS: Beyond the Basics
Three additional factors deserve attention in any discussion of fat survival rates in MTF facial lipofilling. First, hormonal status matters. Estrogen therapy increases subcutaneous fat deposition and promotes angiogenesis—but it also increases thrombotic risk perioperatively. Surgeons must balance the improved vascular environment that estrogen creates at the recipient site against the surgical risks of hormone therapy in the perioperative window. Most protocols recommend continuing estrogen through surgery but using standard venous thromboembolism prophylaxis.
Second, prior filler use complicates fat grafting. Hyaluronic acid fillers, when present in the midface, create a hydrated gel matrix that resists fat incorporation. Injecting fat into filler-laden tissue often produces irregular contours and rapid graft loss as the fat competes for space with the hydrophilic filler material. Surgeons should wait at least six months after hyaluronic acid filler dissolution before placing structural fat grafts. For permanent fillers such as polymethylmethacrylate, the situation is worse—these materials incite chronic inflammation that destroys transplanted adipocytes on contact.
Third, the smoking question cannot be avoided. Nicotine causes peripheral vasoconstriction that directly reduces capillary perfusion at the graft site during the critical revascularization window. Patients who smoke or use nicotine products within two weeks of surgery show measurably lower fat graft survival—one study reported a 28% reduction in retained volume at six months compared to non-smokers. The impact is most severe in thin-tissue areas like the lower eyelid and least pronounced in deep malar fat where native vascularity is robust.
Adipocyte Viability as the Master Variable: Rethinking Fat Grafting Education
The aesthetics industry has invested decades perfecting injection techniques while treating the harvest as an afterthought. Textbook illustrations show elaborate injection patterns but rarely include aspiration pressure on the materials list. Conference workshops teach micro-droplet placement with exquisite detail while the harvesting technician in the corner pulls a syringe plunger with enough force to rupture half the graft. This educational imbalance is the root cause of inconsistent fat survival outcomes worldwide.
The data presented here argues for a fundamental reordering of priorities. Adipocyte viability at harvest should be the first variable every surgeon checks before entering the operating room. If you cannot measure your aspiration pressure, you cannot predict your retention rate. It really is that direct. Low-pressure liposuction devices with built-in manometers cost a fraction of what surgeons spend on marketing—yet they deliver a measurable, patient-visible improvement in outcomes. The technology transition from syringe to controlled suction is not a luxury. It is the single highest-yield intervention available to any practice performing facial fat grafting today.
For transfeminine patients investing in facial feminization, fat graft survival translates directly into confidence, identity alignment, and the avoidance of revision surgeries. Each percentage point of retained volume is one fewer return to the operating room, one less cycle of swelling and waiting and hoping, one more step in a journey that should move forward rather than circle back. The science exists. The equipment exists. The protocol exists. The only variable left is adoption.

Conclusion: Making Fat Survival Predictable in MTF Facial Lipofilling
Fat harvesting pressure is not a minor technical variable—it is the master determinant of adipocyte viability, and by extension, the primary predictor of 12-month volumetric retention in facial lipofilling. Syringe aspiration generates pressures that kill the majority of harvested adipocytes before injection ever begins. Low-pressure liposuction at 250 mmHg preserves viability above 80% and nearly doubles long-term retention. When combined with structured injection techniques—micro-droplet for precision, Coleman for structural depth, and Snodell for triplanar integration—low-pressure harvesting transforms MTF midface augmentation from an unpredictable gamble into a measurable clinical process.
Dr. Mehmet Fatih Okyay and the team at Dr. MFO Clinic have demonstrated that this protocol is not theoretical. Their patient data, measured with 3D volumetric imaging and verified across dozens of transfeminine surgical cases, proves that predictable retention above 60% at twelve months is achievable with disciplined technique. The question is no longer whether low-pressure harvesting works. The question is whether your surgical practice can afford to continue using methods that the evidence has rendered obsolete.
If you are a trans woman considering facial fat grafting as part of your feminization journey, your surgeon’s harvesting protocol will determine whether your results last or fade. Ask about aspiration pressure. Ask about adipocyte viability. Ask to see 3D volumetric retention data. Then contact Dr. MFO Clinic to discuss your surgical plan with a team that measures outcomes rather than guessing at them.
Frequently Asked Questions
How does fat harvesting pressure affect adipocyte viability in facial lipofilling?
Fat harvesting pressure directly impacts adipocyte membrane integrity. High vacuum pressures above 700 mmHg rupture cell membranes through shear forces, reducing viability to roughly 50%. Low-pressure liposuction at 250 mmHg preserves the stromal vascular fraction and maintains adipocyte viability above 80%, which translates into significantly higher long-term graft retention.
What is the difference between syringe aspiration and low-pressure liposuction for fat grafting?
Syringe aspiration generates 700 to 1,200 mmHg of negative pressure manually, causing significant barotrauma to adipocytes. Low-pressure liposuction uses a calibrated suction device at approximately 250 mmHg, gently detaching fat cells while preserving their structural integrity and surrounding stromal vascular fraction, resulting in nearly double the viable cell count.
Why does 12-month volumetric retention matter for MTF midface augmentation?
Twelve-month volumetric retention indicates whether grafted fat has successfully revascularized and integrated permanently. Retention measured by 3D imaging at this milestone distinguishes between initial swelling and true fat survival, giving patients and surgeons reliable data for planning additional procedures or confirming long-term feminization outcomes.
Which injection technique works best for MTF midface fat grafting?
The Snodell triplanar method offers the most comprehensive approach by placing concentrated structural fat deeply, washed fat in the muscular layer, and nanofat superficially. Micro-droplet technique excels for precision in shallow planes, while Coleman structural grafting provides deep volume. Technique selection depends on the specific midface deficit and tissue quality.
How does Dr. MFO Clinic ensure high fat graft survival rates in FFS patients?
Dr. MFO Clinic uses a standardized low-pressure harvesting protocol at 250 mmHg, Coleman centrifugation processing, and the Snodell triplanar injection sequence. Volumetric retention is tracked with 3D surface imaging, and the clinic consistently achieves above 60% retention at twelve months for MTF midface augmentation cases.
What fat reabsorption rate should patients expect after facial lipofilling FFS?
With low-pressure harvesting and proper technique, patients can expect approximately 37% volume loss by twelve months, yielding 63% retention. Syringe-aspiration methods produce approximately 69% volume loss in the same period. These rates are documented through 3D imaging and vary based on hormonal status, smoking, and prior filler use.