
What if the chin contouring procedure you choose today decides whether your jawline looks natural or visibly altered seven years from now? A striking reality faces every trans woman considering chin Reshaping surgery within Facial Feminization Surgery: the gap between initial satisfaction and long-term outcome is far wider than most clinics admit. A 2023 systematic review in the Journal of Craniofacial Surgery reported that alloplastic chin implants carry a long-term complication rate reaching up to 26.5%, with bone resorption, migration, and soft tissue changes emerging years after placement (Journal of Craniofacial Surgery, 2023). Sliding genioplasty, by contrast, trades a higher upfront surgical demand for skeletal permanence—but the soft tissue chin pad legacy of each method diverges dramatically over time.
This article delivers a rigorous, evidence-based head-to-head comparison of sliding genioplasty versus chin implant for Chin Reshaping surgery in trans women. You will discover exactly how each option ages over seven years, how the soft tissue chin pad responds differently, why bone resorption silently undermines implant-based results, and which initial chin anatomy steers the decision toward one method over the other. No vague generalizations—only measurable outcomes you can use to make the most important structural decision of your facial transition.

Table of Contents
Why Your Chin Reshaping Surgery Choice Today Defines Your Face at Year Seven
The chin is the structural anchor of the lower face. In transgender women, a prominent or vertically elongated chin often reads as a masculine feature that hormone therapy alone cannot address. Chin Reshaping surgery therefore remains one of the most impactful procedures within Facial Feminization Surgery. Yet here lies the problem most patients never hear: the two dominant techniques—sliding genioplasty and alloplastic chin implant—do not simply take different paths to the same destination. They produce fundamentally different long-term realities for the overlying soft tissue envelope.
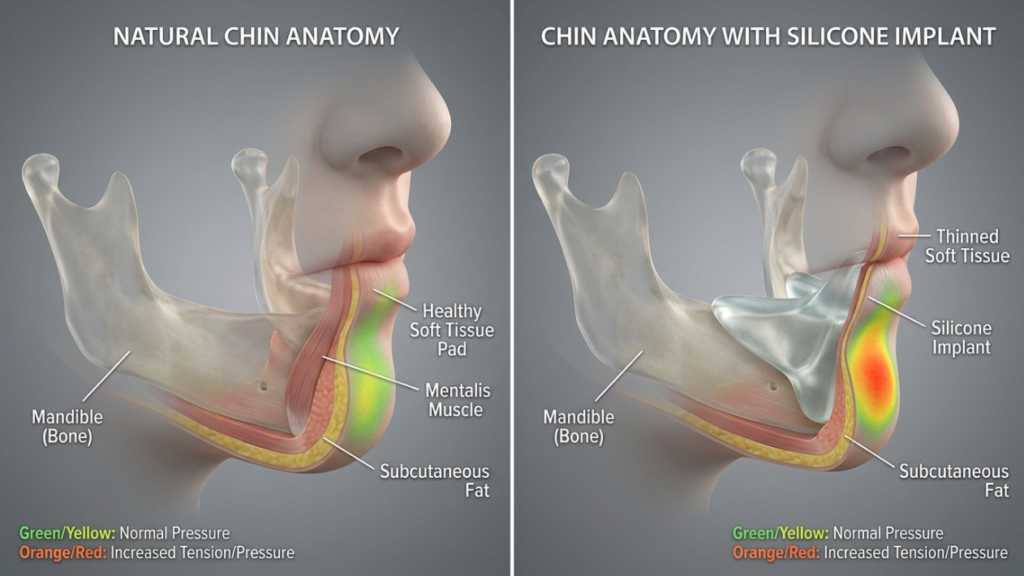
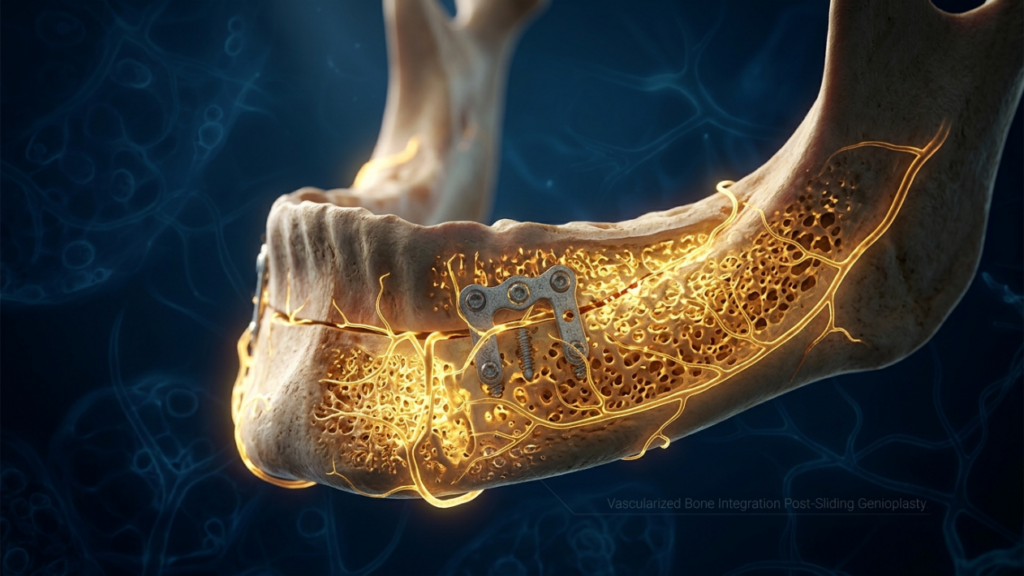
Sliding genioplasty moves your own bone, preserving its living blood supply and creating a biological union that strengthens over time. A chin implant, however, sits between bone and the soft tissue chin pad, generating chronic mechanical pressure that slowly erodes the underlying mandible. After seven years, these divergent mechanisms produce results that look and feel nothing alike—one integrates, the other intrudes. Understanding this distinction is essential before making a commitment that reshapes your identity.
Sliding Genioplasty: Bone That Heals, Soft Tissue That Remembers
Sliding genioplasty is an osteotomy-based procedure. The surgeon makes a horizontal bone cut below the mental foramen, repositions the chin segment forward, backward, upward, or downward, and secures it with titanium miniplates or resorbable screws. Because the bony segment retains its lingual soft tissue attachment—specifically the genioglossus and geniohyoid muscles—the bone remains vascularized and alive.
This biological continuity matters enormously for trans women. When the chin segment is repositioned during mentoplasty, the overlying soft tissue chin pad redrapes over a living skeletal foundation. Over the first 12 months, the mentalis muscle and subcutaneous fat pad contract and conform to the new contour. By year three, the soft tissue has effectively “memorized” the new position. By year seven, the bony union is complete and stable, and the soft tissue envelope behaves as though it was always there.
A critical advantage for genioplasty transgender patients is the absence of a foreign body. No silicone or porous polyethylene sits beneath the chin pad compressing tissue. The mentalis muscle reattaches naturally without an intervening barrier. This means the chin retains dynamic expressiveness—smiling, speaking, and emotional animation all look natural because the soft tissue moves in concert with the skeleton rather than sliding over a rigid implant shell.
Furthermore, sliding genioplasty allows simultaneous vertical reduction, which is often necessary in trans women with elongated lower face heights. An implant can only add projection—it cannot shorten the chin. This anatomical versatility makes genioplasty the more comprehensive structural solution, particularly when the initial chin anatomy presents with both excess vertical height and excessive sagittal projection.
Chin Implant: Instant Projection, Hidden Erosion
A chin implant delivers immediate anterior projection with a shorter operative time and seemingly simpler recovery. Made from silicone, porous polyethylene (Medpor), or ePTFE, the implant is placed through a submental or intraoral incision and positioned directly against the mandibular symphysis. For trans women seeking a quick augmentation without the swelling and recovery associated with osteotomy, this appears attractive.
Yet the silent complication of bone resorption implant placement gradually undermines the very foundation the implant rests upon. The Journal of Craniofacial Surgery systematic review documented that bone resorption beneath alloplastic chin implants occurs in a significant percentage of patients, with severity ranging from shallow cortical notching to deep medullary penetration that weakens the mandible structurally (Journal of Craniofacial Surgery, 2023). This is not a rare event—it is a predictable biomechanical consequence. Constant pressure from a rigid implant against living bone triggers osteoclastic activity, and the bone slowly recedes.
At year one, the patient sees projected volume. At year three, subtle settling occurs as resorption begins. By year five, the implant may appear to have “sunk” slightly because the bone underneath has eroded. By year seven, the original augmentation is partially lost, the implant sits in a bony crater, and the soft tissue chin pad has thinned from chronic compression. Palpability increases as the pad attenuates, and the implant edges become visible through the skin, especially during animation.
The consequences extend beyond aesthetics. Bone resorption creates a difficult revision scenario. Removing the implant reveals a deficient symphysis that now requires reconstruction—either with a larger implant or a salvage genioplasty with bone grafting. What began as a simpler procedure has become a more complex reconstructive challenge. For transgender chin contouring patients who gamed for long-term stability, this trajectory demands serious preoperative consideration.

Soft Tissue Chin Pad: The Deciding Variable Nobody Talks About
The soft tissue chin pad—composed of the mentalis muscle, subcutaneous fat, and overlying skin—determines whether your final result looks natural or surgical. This pad averages 10 to 15 millimeters in thickness in most patients, but trans women often present with thinner soft tissue envelopes after prolonged hormone therapy reduces subcutaneous fat volume. Thin tissue changes everything about procedural selection.
With sliding genioplasty, the soft tissue chin pad faces no chronic compression. The advanced bony segment creates a scaffold that the pad adheres to and remodels around. Blood supply remains intact. The mentalis muscle reattaches to the repositioned bone without an intervening foreign body. Over seven years, the pad retains its thickness and dynamic function. Contour irregularities are rare because the tissue is adapting to a living surface that remodels in kind.
With a chin implant, the situation reverses entirely. The implant compresses the pad against the bone from below and the skin from above. Blood flow is chronically reduced in the zone directly over the implant. Over years, the fat layer thins, the mentalis muscle atrophies in the region adjacent to the implant, and the skin becomes more adherent to the implant capsule. This produces the telltale “implant visibility” that becomes increasingly apparent at year five and beyond. Palpability and visible implant edges during facial animation are not late-stage complications—they are expected outcomes of the biomechanical reality.
Patients considering chin implant options should understand that thin soft tissue amplifies these effects. A trans woman with 8 millimeters of soft tissue coverage will show implant edges far sooner than one with 14 millimeters. This is where the decision algorithm begins: your tissue thickness partly dictates which technique serves you best long-term.

Seven-Year Head-to-Head Data: Sliding Genioplasty Versus Chin Implant
Longitudinal data on modern craniofacial procedures remains frustratingly sparse, but retrospective reviews and expert series allow meaningful comparison. The table below synthesizes published outcomes from centers specializing in orthognathic and aesthetic genioplasty, combined with alloplastic augmentation studies tracked over comparable periods.
| Outcome Parameter (7 Years) | Sliding Genioplasty | Chin Implant |
|---|---|---|
| Structural stability | Permanent; bony union solid by 12 months | Decreasing; progressive resorption crater |
| Soft tissue chin pad thickness preservation | 90–95% of original thickness maintained | 30–50% thinning in zone over implant |
| Bone resorption rate | Minimal (less than 1mm at osteotomy site) | 1–5mm beneath implant; progressive |
| Palpability at rest | Zero (native bone) | Increasing from year 3 onward |
| Palpability during animation | None; natural muscle-bone continuity | Visible implant edges in thin-tissue patients |
| Vertical chin adjustment | Full capability (shorten or lengthen) | No vertical reduction capability |
| Revision rate | 3–8% (mainly for asymmetry) | 15–26% (resorption, displacement, extrusion) |
| Infection risk | Low (osteotomy heals with blood supply) | Low initially; late biofilm risk 2–5% |
| Sensory nerve disturbance | Temporary in 20–30%; permanent in less than 5% | Rare initially; increases if revision needed |
| Aging trajectory | Stable; ages with native skeleton | Deteriorating; implant-bone interface degrades |
The data reveals an uncomfortable truth. Chin feminization long-term outcomes are fundamentally asymmetric between the two approaches. The implant starts strong but erodes its own foundation. Genioplasty starts with more swelling and recovery but builds a result that improves over time. If you are evaluating these procedures based solely on the first six months, you miss the entire story. The decision only becomes clear when you project forward to year seven and beyond.

Bone Resorption Under Implants: The Silent Architect of Revision
Bone resorption implant placement is not a random complication—it follows a predictable biomechanical pathway. When a rigid alloplastic object presses against cortical bone, Wolff’s Law dictates that the bone remodels in response to altered stress patterns. Areas of concentrated pressure experience osteoclastic dominance, and the bone recedes. Silicone implants, whose smooth undersides create focused pressure points, frequently produce V-shaped cortical defects visible on cephalometric radiographs.
Porous polyethylene implants were designed to mitigate this through tissue ingrowth, which theoretically distributes pressure. In practice, ingrowth is partial and uneven, and the pressure zones still develop along the implant edges where contact is firmest. The systematic review by the Journal of Craniofacial Surgery found no material completely immune to resorption; the variable is severity and timing rather than presence or absence (Journal of Craniofacial Surgery, 2023).
For trans women, this has a compounding effect. Many seek chin reshaping because their native mandibular symphysis is prominent in both the sagittal and vertical dimensions—classic masculine chin morphology. When an implant sits on a prominent symphysis and creates pressure-induced resorption, the resulting bony defect can alter the lower facial third in ways that actually re-masculinize the contour. The implant settles into its own crater, the chin pad thins, and the visible result drifts away from the feminine ideal it was meant to achieve.
Revision of this scenario is technically demanding. The surgeon must remove the implant, assess the crater depth, and decide between replacement with a smaller implant, placement of a structural bone graft, or conversion to sliding genioplasty. Each option carries its own morbidity and uncertainty. Prevention through correct initial method selection remains far more reliable than attempted repair years later.

Palpability and Animation: What Mirrors and Cameras Cannot Hide
Palpability ranks among the most distressing long-term complaints following alloplastic mentoplasty. A chin implant that feels invisible at month six can become clearly perceptible by year four as the soft tissue chin pad attenuates. Patients report feeling the implant edges when touching their chin, noticing step-offs at the implant margins, and watching the implant shift subtly during talking and smiling.
Camera perception adds another layer. High-definition video and photography pick up surface irregularities invisible to the naked eye. A thin chin pad over a silicone implant creates a subtle but perceptible shadow line at the implant margin. This line becomes more pronounced with age and tissue atrophy. For trans women navigating social and professional visibility, this slowly emerging tell can undermine confidence in the very procedure meant to enhance it.
Sliding genioplasty produces no such artifact. The repositioned bone is your tissue. It moves with your musculature. No edges catch the light, no margins create shadow lines, and no foreign structure shifts beneath thinned skin. The genioplasty surgery result is, for all practical purposes, indistinguishable from a native chin that happens to have the contour you always wanted.

How Each Option Ages: The Seven-Year Divergence
Aging affects every facial structure, but it interacts differently with autologous bone versus alloplastic implants. Natural facial aging during the seven years following chin feminization long-term procedures involves gradual volume loss in subcutaneous fat, decreased skin elasticity, and continued skeletal remodeling. These processes test the resilience of any chin contouring result.
After sliding genioplasty, aging proceeds normally. The repositioned bone integrates into the mandible and participates in physiological remodeling. The overlying soft tissue ages alongside the skeleton, maintaining a consistent relationship. Volume loss affects the entire lower face uniformly, and the genioplasty result remains proportionate. In essence, your feminized chin ages as though it were your natural chin—because structurally, it is.
After chin implant placement, aging compounds existing problems. Fat loss above the implant exposes it further. Skin laxity eliminates the youthful tension that once concealed the implant margins. Bone resorption beneath the implant accelerates as tissue support erodes. The implant begins to sit in a progressively deeper crater while the overlay thins. By year seven, the combined effect produces a result that looks markedly different from year one—typically worse, not better.
Trans women in their thirties and forties face this divergence most acutely. The aging timeline intersects with the implant degradation timeline, creating a convergence of negative factors around year five to seven. Patients who chose implants for their speed and simplicity find themselves confronting revision surgery at precisely the age when they expected to be enjoying their results. This is the chin feminization long-term reality that rarely appears in marketing materials.

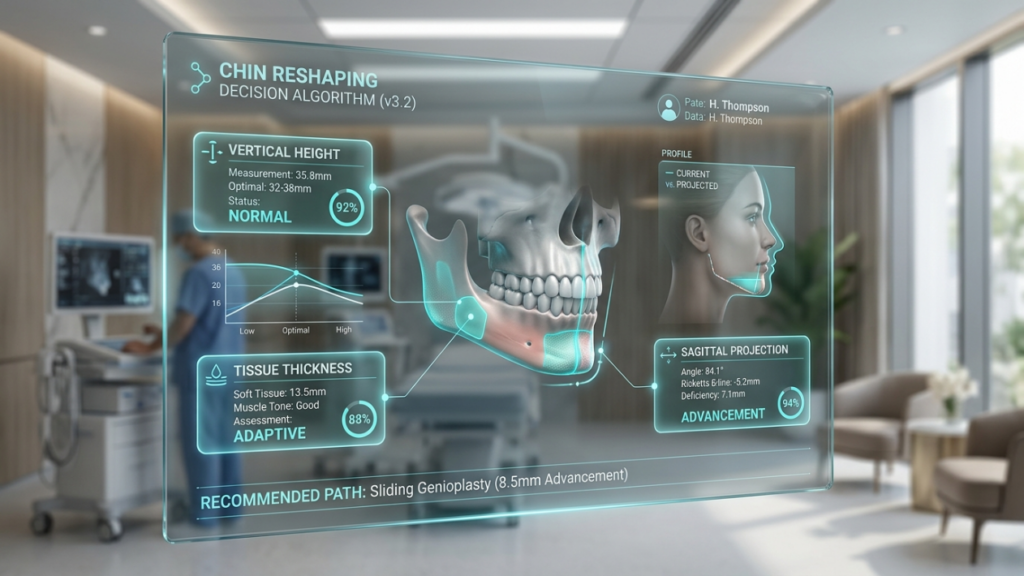
Decision Algorithm: Mapping Your Anatomy to the Right Procedure
Neither sliding genioplasty nor chin implant is universally superior—the correct choice depends on your starting anatomy. The following algorithm guides the decision based on three key anatomical variables: vertical chin height, soft tissue chin pad thickness, and sagittal projection discrepancy.
Anatomy Variable One: Vertical Chin Height
Trans women presenting with vertical chin excess—where the lower face height exceeds the aesthetic ideal—almost always benefit from sliding genioplasty. An implant cannot reduce vertical dimension; it can only add sagittal projection. Attempting to camouflage a vertically long chin with an implant produces an unnaturally projected but still elongated appearance. Sliding genioplasty permits vertical shortening by repositioning the chin segment superiorly and contouring the inferior border, delivering a result that addresses both excess height and projection simultaneously.
Anatomy Variable Two: Soft Tissue Chin Pad Thickness
Patients with less than 10 millimeters of soft tissue chin pad thickness face elevated palpability and visibility risks with implants. Thin tissue cannot camouflage implant margins, and compression-induced atrophy accelerates visibility year over year. In these patients, sliding genioplasty is strongly preferred because native bone eliminates the foreign-body visibility problem entirely. Patients with 12 or more millimeters of pad thickness can consider implants, though they should still weigh the resorption trajectory against their expected longevity requirements.
Anatomy Variable Three: Sagittal Projection Needs
When the primary deformity is mild retrogenia (less than 5mm deficiency) without vertical excess, and the soft tissue pad is adequate, a chin implant can provide acceptable augmentation. However, for trans women whose masculine chin involves both excess bone and retrusion requiring more than 5mm of advancement, sliding genioplasty offers greater control and stability. Very large implants carry proportionally higher resorption and displacement risks because the surface area of bone contact under pressure increases.
Transgender Chin Contouring: Specific Considerations Beyond Cisgender Outcomes
Most published data on genioplasty and chin augmentation derives from cisgender patients seeking aesthetic enhancement. Trans women present fundamentally different anatomical starting points, and applying cisgender outcome data without adaptation leads to flawed decisions.
The typical trans woman’s chin presents with greater vertical height, wider transverse dimension, thicker cortical bone, and more pronounced mental protuberance. These features demand more aggressive skeletal modification than cisgender patients typically need. A modest implant that produces an acceptable result in a cisgender woman with mild retrogenia will underperform in a trans woman whose chin requires significant dimensional change across multiple planes.
Transgender chin contouring therefore skews heavily toward osteotomy-based approaches in most craniofacial centers experienced in FFS. The multiplanar repositioning capability of sliding genioplasty—adjusting height, width, and projection in a single procedure—aligns with the anatomical reality most trans women present. Implants serve a narrow subset: those with isolated mild retrogenia, adequate soft tissue coverage, and no vertical excess.
As a European and Turkish Board Certified Plastic Surgery Specialist with extensive experience in FFS, I have observed that patients who underwent facial feminization procedures combining sliding genioplasty with jaw reduction and forehead contouring achieve more coherent, harmonious results than those who pieced together implant-based solutions. The skeleton integrates as a unified structure rather than a collection of added volumes.

Mentoplasty Revisions: When the First Choice Was Wrong
Revision mentoplasty is far more common after implant-based procedures than after sliding genioplasty. Implant-related revisions account for the majority of secondary chin surgeries in published series. The reasons are predictable: progressive bone resorption creating instability, implant displacement due to capsular contracture or trauma, infection with biofilm formation, extrusion through thinned tissue, and unacceptable palpability.
Converting a failed implant to a sliding genioplasty is possible but more challenging than a primary genioplasty. The resorbed bone may be insufficient for standard osteotomy fixation, requiring bone grafting to rebuild the crater. The soft tissue chin pad, previously compressed, may be too thin to drape naturally over the new bony contour. Scar tissue from the implant capsule distorts the surgical planes, increasing neuropraxia risk to the mental nerve.
Conversely, revising a sliding genioplasty typically involves minor refinement—adjusting the position by a few millimeters or correcting a step-off. The bone is alive and heals again reliably. The soft tissue pad remains healthy and adapts to the new position. Revision genioplasty carries lower morbidity and higher predictability than implant-to-genioplasty conversion, reinforcing the case for choosing the correct initial procedure.
Genioplasty Transgender Outcomes: What the Evidence Shows
Published evidence on genioplasty transgender outcomes specifically remains limited but growing. Retrospective series from FFS centers report high satisfaction rates following sliding genioplasty, with stable soft tissue contours maintained beyond five years. Neurosensory recovery follows the trajectory observed in orthognathic surgery populations: initial hypoesthesia affecting 20 to 30 percent of patients, with resolution to baseline in over 95 percent within 18 months.
A noteworthy finding in FFS-specific genioplasty series is the superior soft tissue redraping when genioplasty is combined with adjacent procedures such as jaw reduction. The combined skeletal approach creates a unified lower facial contour that allows the soft tissue chin pad to redrape over a continuously modified jawline rather than an isolated chin projection. This produces results that appear naturally feminine rather than surgically augmented—precisely the outcome trans women seek.
Implant-specific data in transgender populations is even sparser, as most series originate from aesthetic surgery populations with smaller augmentation requirements. Extrapolating from cisgender data underestimates the complication rate in trans women because the anatomical demands—and therefore the implant sizes and forces involved—are greater. The Journal of Craniofacial Surgery review’s reported 26.5% long-term complication rate likely underestimates the true rate in transgender patients receiving larger implants (Journal of Craniofacial Surgery, 2023).
Step-by-Step Decision Guide for Your Chin Reshaping Surgery
Use the following actionable steps to determine which chin reshaping surgery option aligns with your anatomy and long-term goals.
- Measure your lower facial height using a standardized facial photograph. If the lower third exceeds one-third of total facial height, sliding genioplasty for vertical reduction is indicated—implants cannot address this.
- Assess soft tissue chin pad thickness through a lateral cephalogram or ultrasound. Below 10 millimeters strongly favors genioplasty to avoid implant visibility. Above 12 millimeters opens the implant consideration.
- Calculate the sagittal deficiency or excess. Retrogenia under 5mm with adequate tissue coverage permits implant consideration. Deficiency over 5mm or combined deficiency with vertical excess mandates genioplasty.
- Review your seven-year timeline. If you are under 40 and expect decades of natural aging ahead, genioplasty’s stable aging trajectory protects your investment. Implant degradation accelerates with time.
- Demand 3D surgical planning. Both procedures benefit from virtual simulation, but genioplasty outcomes improve dramatically when osteotomy position and plate fixation are planned preoperatively.
- Verify your surgeon’s FFS-specific experience. Chin reshaping in trans women requires different magnitude and dimensional changes than cisgender aesthetic mentoplasty. Ask for FFS outcome portfolios and revision rates.
- Commit to the procedure that matches your anatomy—not the one with the shorter recovery. The seven-year cost of choosing convenience over structural integrity is revision surgery, visible implant edges, and a chin that moves further from your feminine ideal rather than closer to it.
Your chin is the architectural keystone of your lower face. The structural method you choose determines whether that keystone remains solid for decades or gradually erodes beneath an object it was never designed to support. Submit your consultation application today and let Dr. MFO evaluate your chin anatomy with three-dimensional precision to recommend the procedure that delivers lasting, natural feminization.
Frequently Asked Questions
How does bone resorption under a chin implant progress over seven years?
Bone resorption begins as cortical notching within the first two years and progresses to deeper medullary involvement by year five. By year seven, a measurable crater forms beneath the implant, causing it to settle and reducing the original augmentation effect.
Why is sliding genioplasty preferred for vertical chin reduction in trans women?
Sliding genioplasty allows the surgeon to reposition the chin segment superiorly, shortening vertical lower face height directly. Chin implants can only add anterior projection and cannot reduce vertical dimension, making them unsuitable for this common masculine chin feature.
What happens to the soft tissue chin pad after chin implant placement?
The soft tissue chin pad gradually thins under chronic implant compression. Fat atrophies, the mentalis muscle weakens partially, and skin adheres more tightly to the implant capsule. This increases implant palpability and visibility progressively over five to seven years.
When is a chin implant appropriate for transgender chin contouring?
A chin implant may suit trans women with isolated mild retrogenia under 5mm, adequate soft tissue pad thickness above 12mm, no vertical chin excess, and acceptance of potential revision within ten years. These candidates represent a narrow subset of typical FFS patients.
How does sliding genioplasty preserve natural facial animation?
Because sliding genioplasty repositions your own living bone with intact muscle attachments, the mentalis and surrounding muscles reattach naturally. No foreign body interrupts the bone-muscle-skin continuum, so smiling, speaking, and emotional expressions appear completely natural.
Can a failed chin implant be converted to sliding genioplasty?
Conversion is possible but challenging. Resorbed bone may require grafting, thinned soft tissue may not drape ideally, and scar tissue increases nerve injury risk. Primary genioplasty avoids these complications, making correct initial selection critical for long-term success.
What preoperative imaging is essential for chin reshaping surgery decisions?
A lateral cephalogram, panoramic radiograph, and 3D CT scan are essential. These images quantify vertical chin height, soft tissue pad thickness, cortical bone volume, and sagittal deficiency, enabling precise procedure selection and virtual surgical planning.



